

Native contrast visualization and tissue characterization of myocardial radiofrequency ablation and acetic acid chemoablation lesions at 0.55 T
- PMID: 33952312
- PMCID: PMC8101152
- DOI: 10.1186/s12968-020-00693-1
Native contrast visualization and tissue characterization of myocardial radiofrequency ablation and acetic acid chemoablation lesions at 0.55 T
Abstract
Purpose: Low-field (0.55 T) high-performance cardiovascular magnetic resonance (CMR) is an attractive platform for CMR-guided intervention as device heating is reduced around 7.5-fold compared to 1.5 T. This work determines the feasibility of visualizing cardiac radiofrequency (RF) ablation lesions at low field CMR and explores a novel alternative method for targeted tissue destruction: acetic acid chemoablation.
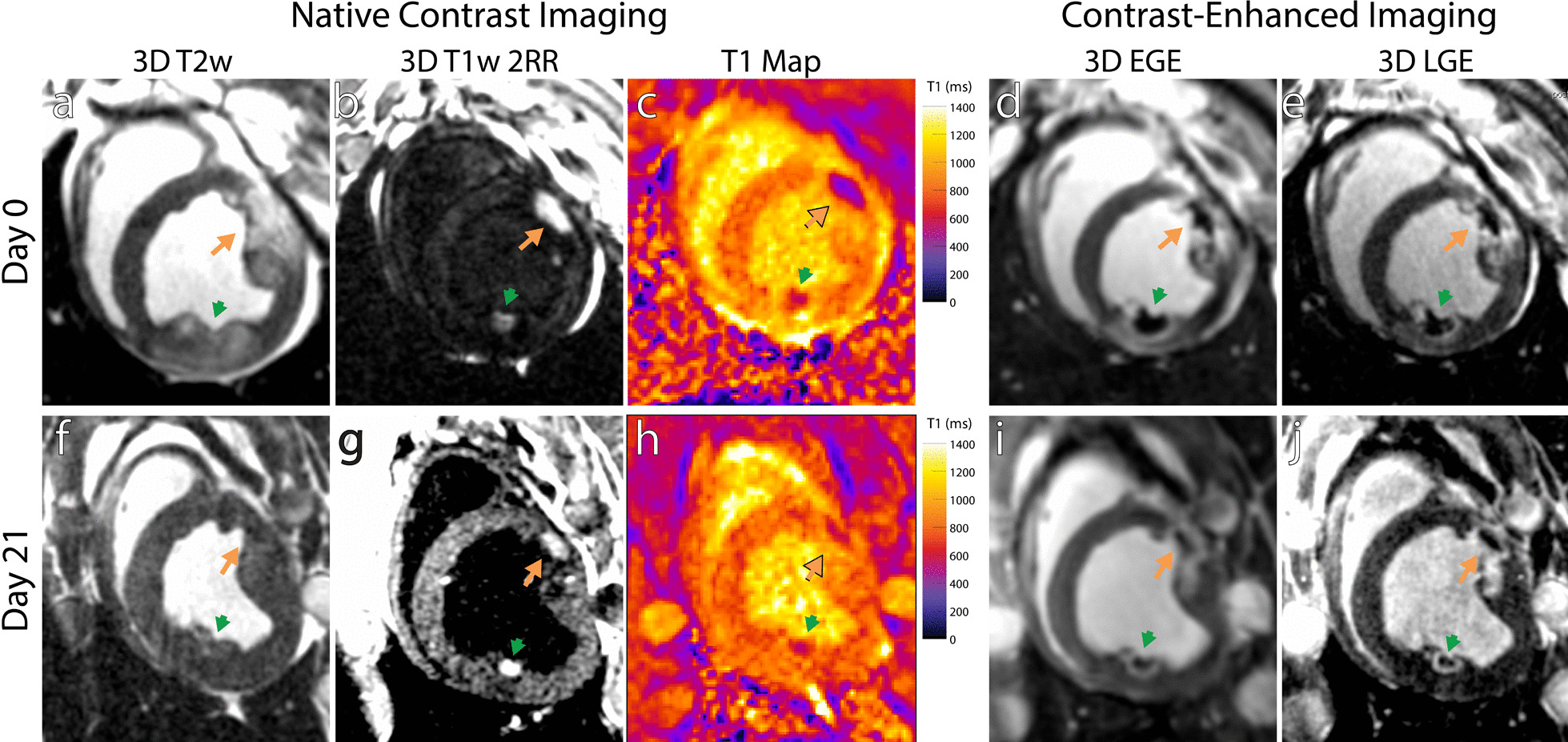
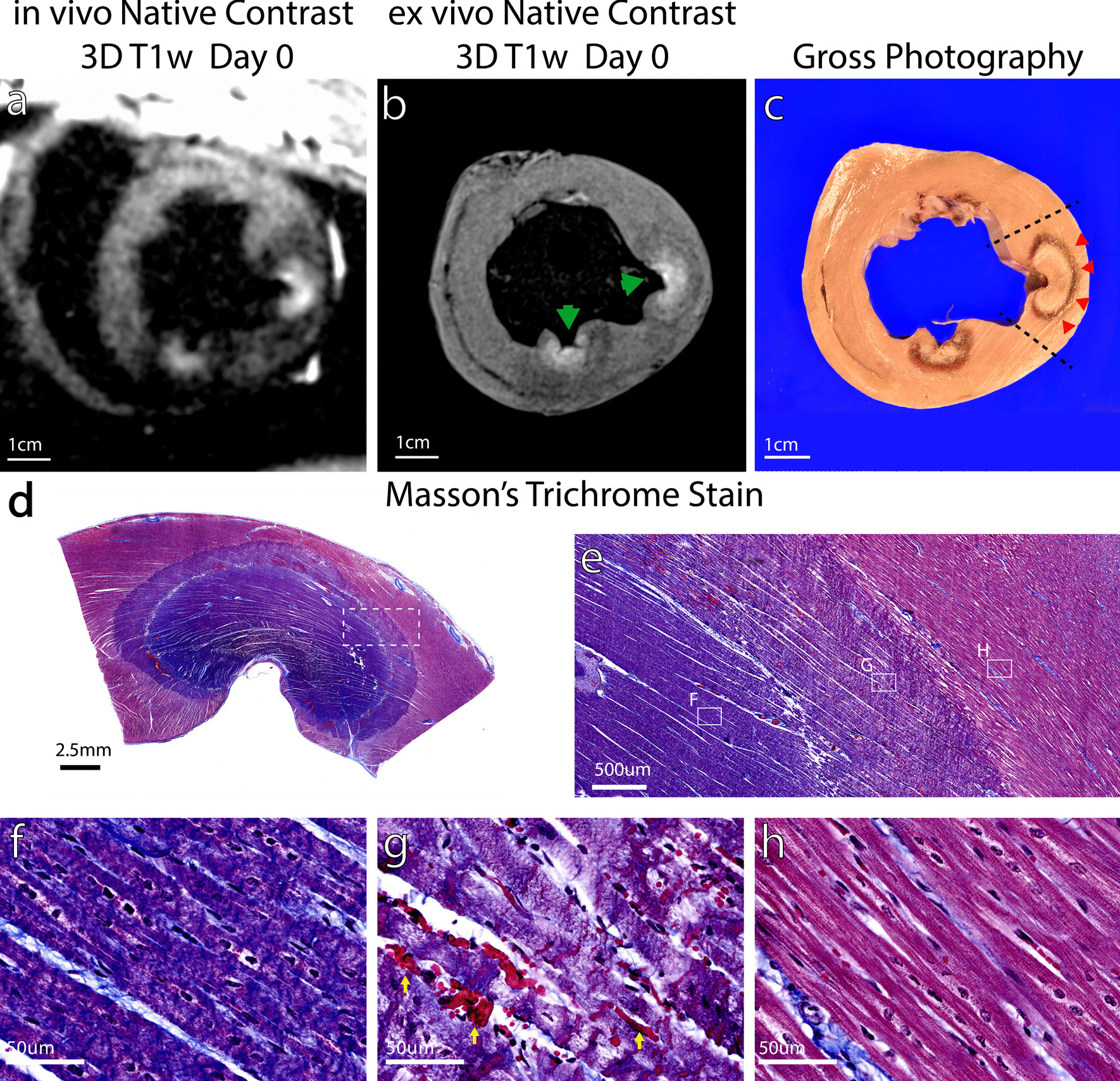
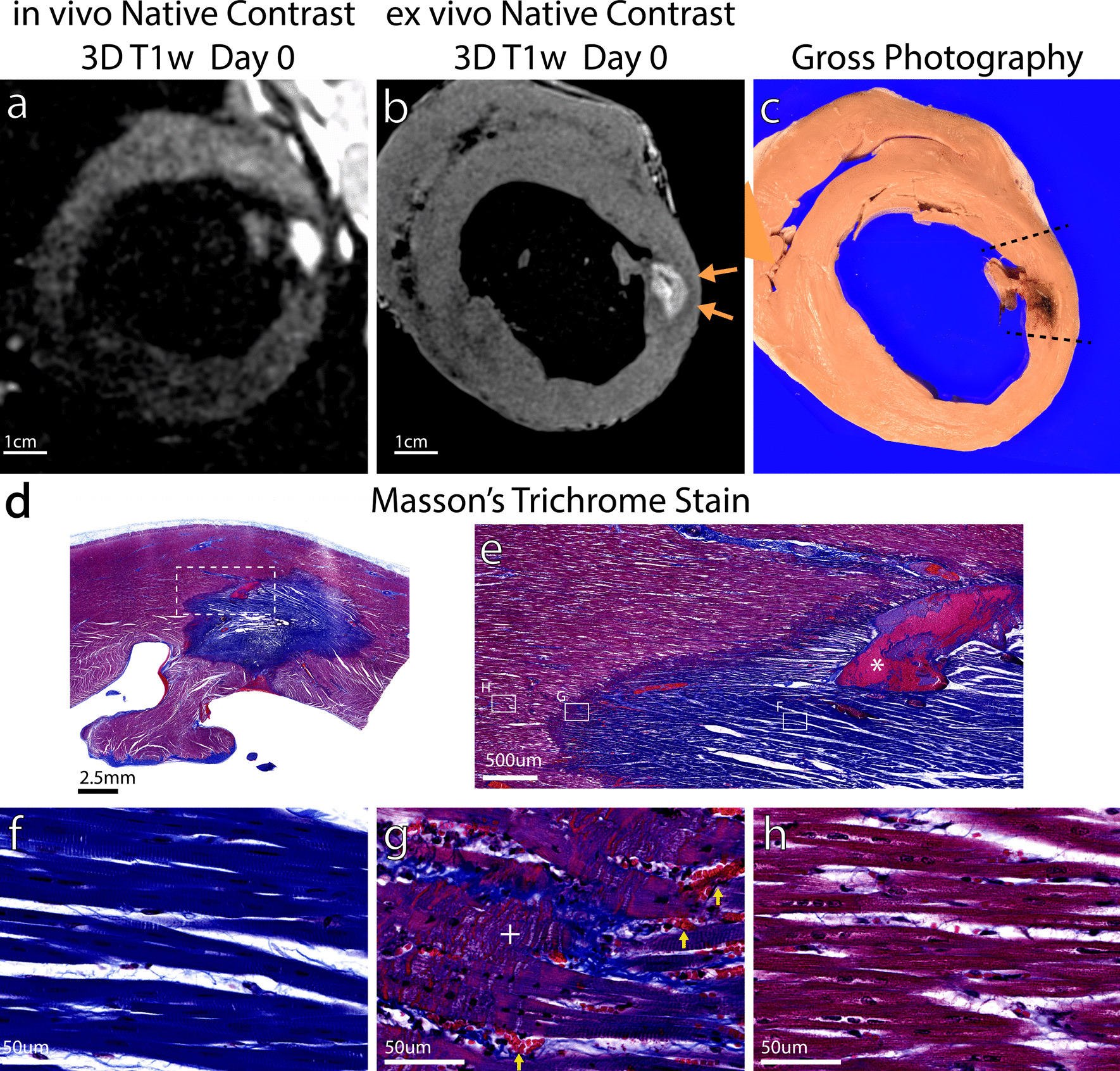
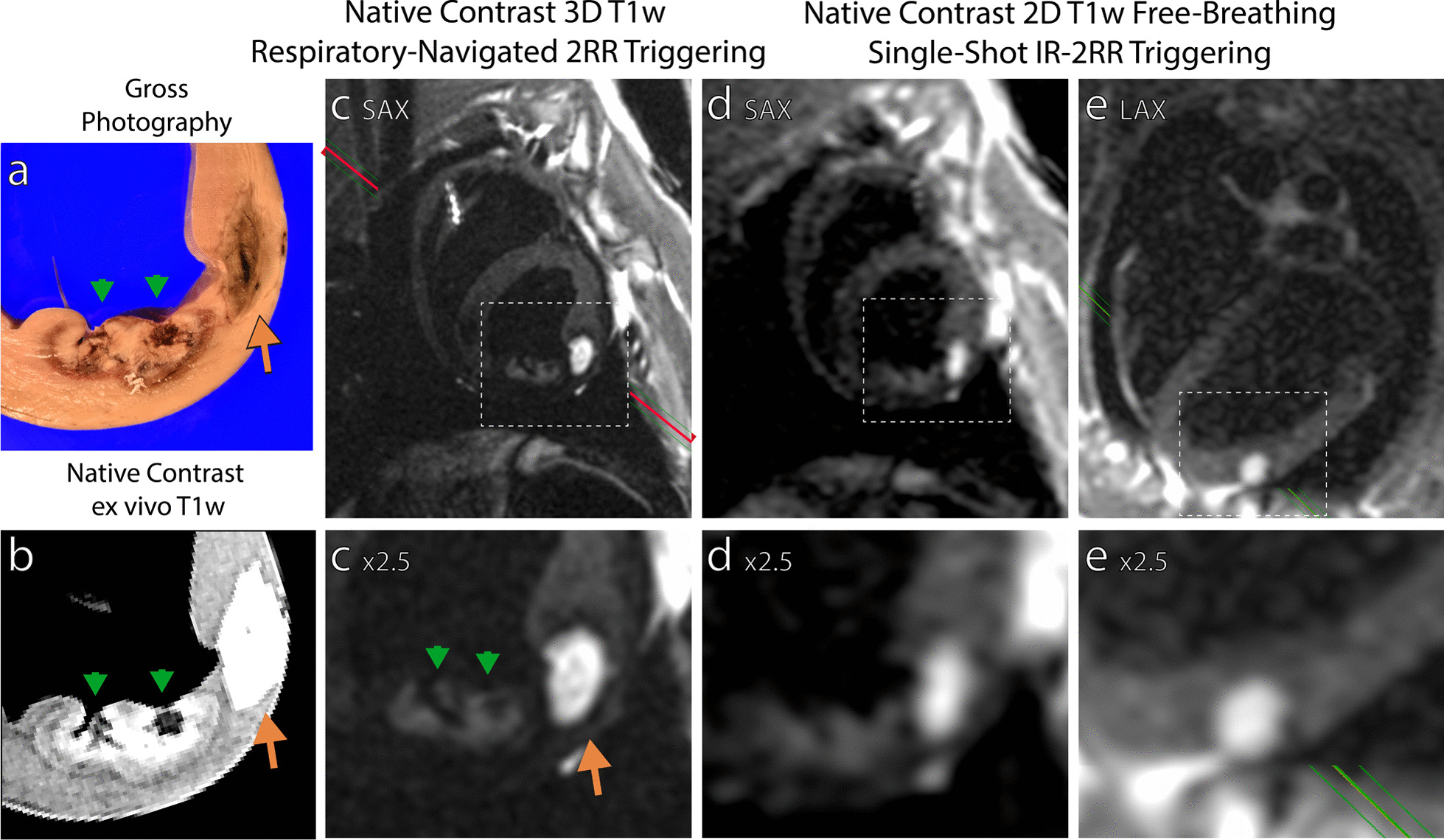
Methods: N = 10 swine underwent X-ray fluoroscopy-guided RF ablation (6-7 lesions) and acetic acid chemoablation (2-3 lesions) of the left ventricle. Animals were imaged at 0.55 T with native contrast 3D-navigator gated T1-weighted T1w) CMR for lesion visualization, gated single-shot imaging to determine potential for real-time visualization of lesion formation, and T1 mapping to measure change in T1 in response to ablation. Seven animals were euthanized on ablation day and hearts imaged ex vivo. The remaining animals were imaged again in vivo at 21 days post ablation to observe lesion evolution.
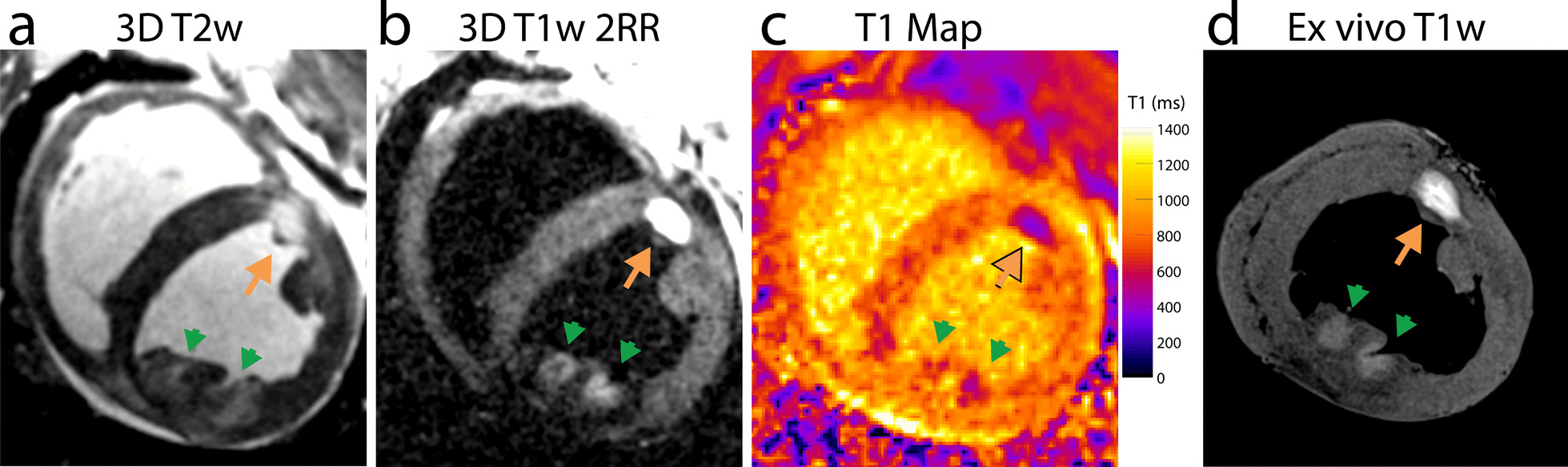
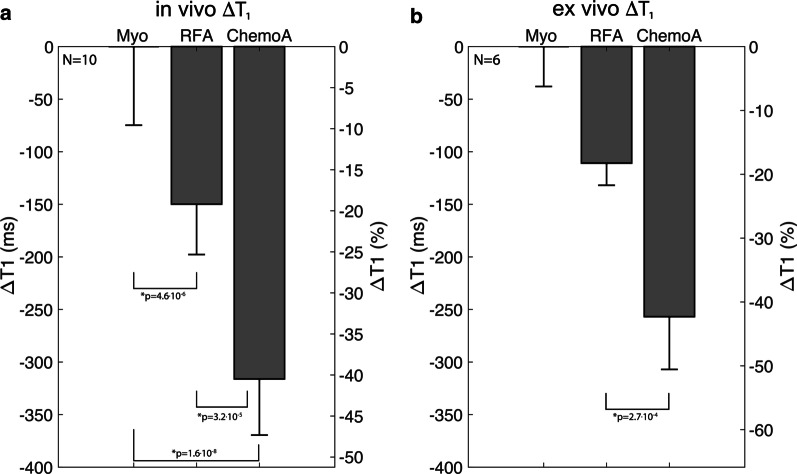
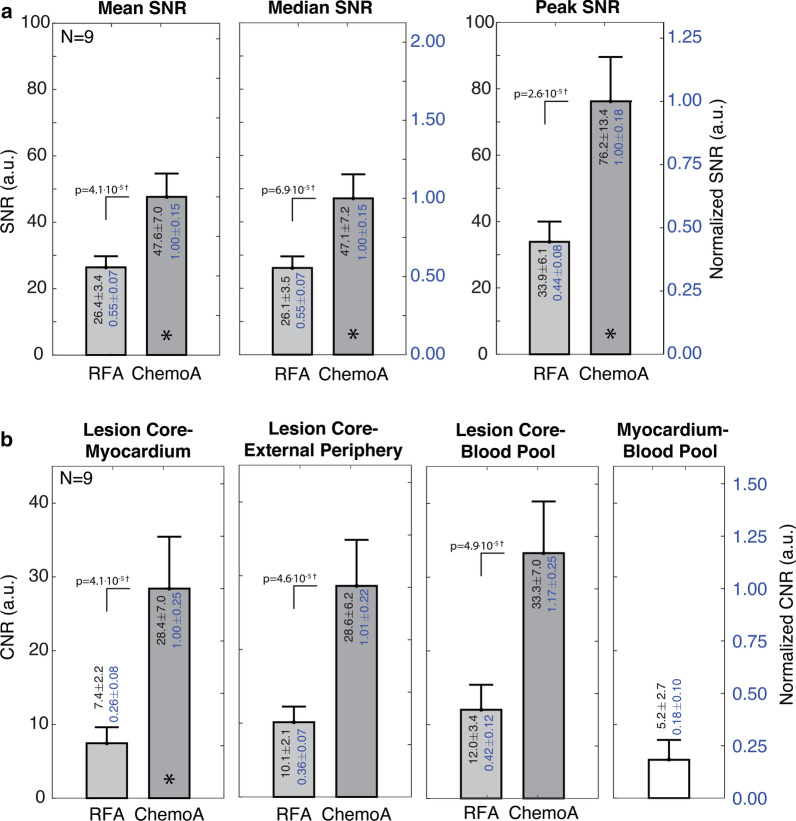
Results: Chemoablation lesions could be visualized and displayed much higher contrast than necrotic RF ablation lesions with T1w imaging. On the day of ablation, in vivo myocardial T1 dropped by 19 ± 7% in RF ablation lesion cores, and by 40 ± 7% in chemoablation lesion cores (p < 4e-5). In high resolution ex vivo imaging, with reduced partial volume effects, lesion core T1 dropped by 18 ± 3% and 42 ± 6% for RF and chemoablation, respectively. Mean, median, and peak lesion signal-to-noise ratio (SNR) were all at least 75% higher with chemoablation. Lesion core to myocardium contrast-to-noise (CNR) was 3.8 × higher for chemoablation. Correlation between in vivo and ex vivo CMR and histology indicated that the periphery of RF ablation lesions do not exhibit changes in T1 while the entire extent of chemoablation exhibits T1 changes. Correlation of T1w enhancing lesion volumes indicated in vivo estimates of lesion volume are accurate for chemoablation but underestimate extent of necrosis for RF ablation.
Conclusion: The visualization of coagulation necrosis from cardiac ablation is feasible using low-field high-performance CMR. Chemoablation produced a more pronounced change in lesion T1 than RF ablation, increasing SNR and CNR and thereby making it easier to visualize in both 3D navigator-gated and real-time CMR and more suitable for low-field imaging.
Keywords: Arrhythmias; Catheter ablation; Chemoablation; Heart; Image-guided intervention; Myocardial ablation; RF ablation; Tissue characterization.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Dinov B, Fiedler L, Schonbauer R, Bollmann A, Rolf S, Piorkowski C, et al. Outcomes in catheter ablation of ventricular tachycardia in dilated nonischemic cardiomyopathy compared with ischemic cardiomyopathy: results from the Prospective Heart Centre of Leipzig VT (HELP-VT) Study. Circulation. 2014;129(7):728–736. doi: 10.1161/CIRCULATIONAHA.113.003063. - DOI - PubMed
-
- Cheung JW, Yeo I, Ip JE, Thomas G, Liu CF, Markowitz SM, et al. Outcomes, costs, and 30-day readmissions after catheter ablation of myocardial infarct-associated ventricular tachycardia in the real world: nationwide readmissions database 2010 to 2015. Circ Arrhythm Electrophysiol. 2018;11(11):e006754. doi: 10.1161/CIRCEP.118.006754. - DOI - PubMed
-
- Bogun FM, Desjardins B, Good E, Gupta S, Crawford T, Oral H, et al. Delayed-enhanced magnetic resonance imaging in nonischemic cardiomyopathy: utility for identifying the ventricular arrhythmia substrate. J Am Coll Cardiol. 2009;53(13):1138–1145. doi: 10.1016/j.jacc.2008.11.052. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
