

Quality of life and healthcare utilisation improvements after atrial fibrillation ablation
- PMID: 33952593
- PMCID: PMC8327410
- DOI: 10.1136/heartjnl-2020-318676
Quality of life and healthcare utilisation improvements after atrial fibrillation ablation
Abstract
Objective: Pulmonary vein isolation (PVI) guided by a standardised CLOSE (contiguous optimised lesions) protocol has been shown to increase clinical success after catheter ablation for paroxysmal atrial fibrillation (PAF). This study analysed healthcare utilisation and quality of life (QOL) outcomes from a large multicentre prospective study, measured association between QOL and atrial fibrillation (AF) burden and identified factors associated with lack of QOL improvement.
Methods: CLOSE-guided ablation was performed in 329 consecutive patients (age 61.4 years, 60.8% male) with drug-refractory PAF in 17 European centres. QOL was measured at baseline and 12 months post-ablation via Atrial Fibrillation Effect on QualiTy of Life Survey (AFEQT) and EuroQoL EQ-5D-5L questionnaires. All-cause and cardiovascular hospitalisations and cardioversions over 12 months pre-ablation and post-ablation were recorded. Rhythm monitoring included weekly and symptom-driven trans-telephonic monitoring, plus ECG and Holter monitoring at 3, 6 and 12 months. AF burden was defined as the percentage of postblanking tracings with an atrial tachyarrhythmia ≥30 s. Continuous measures across multiple time points were analysed using paired t-tests, and associations between various continuous measures were analysed using independent sample t-tests. Each statistical test used two-sided p values with a significance level of 0.05.
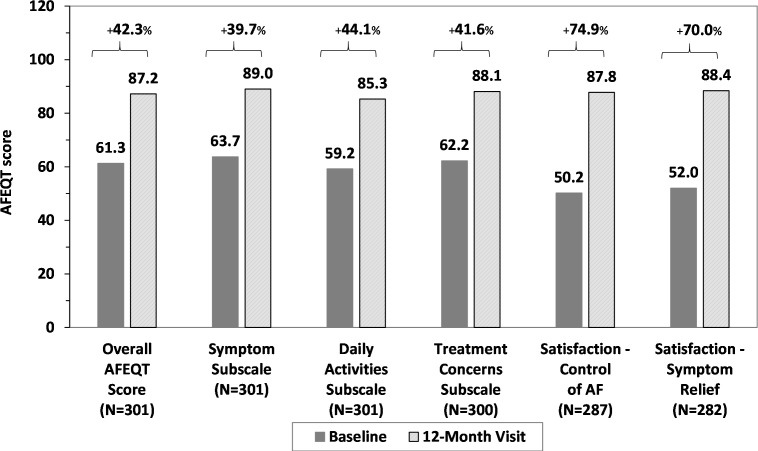
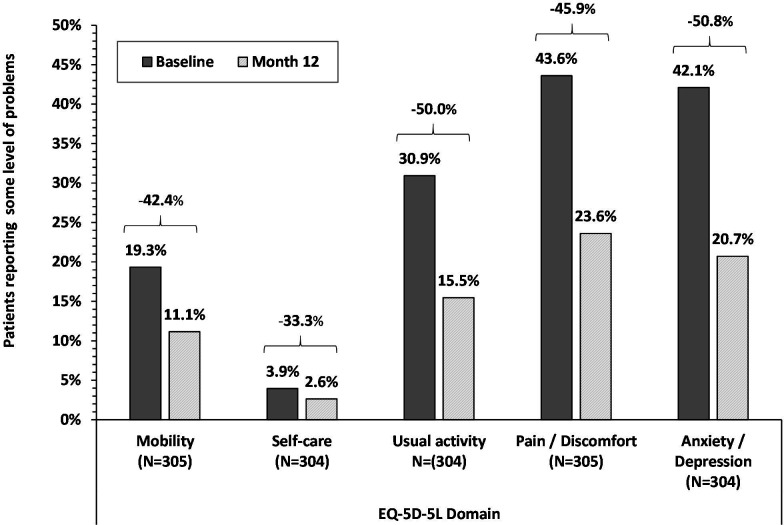
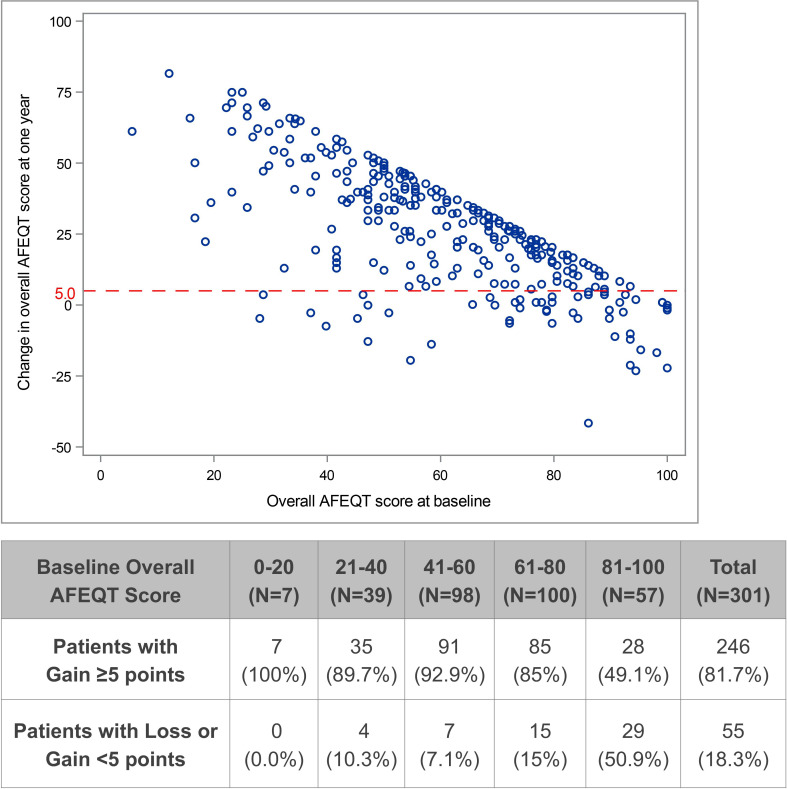
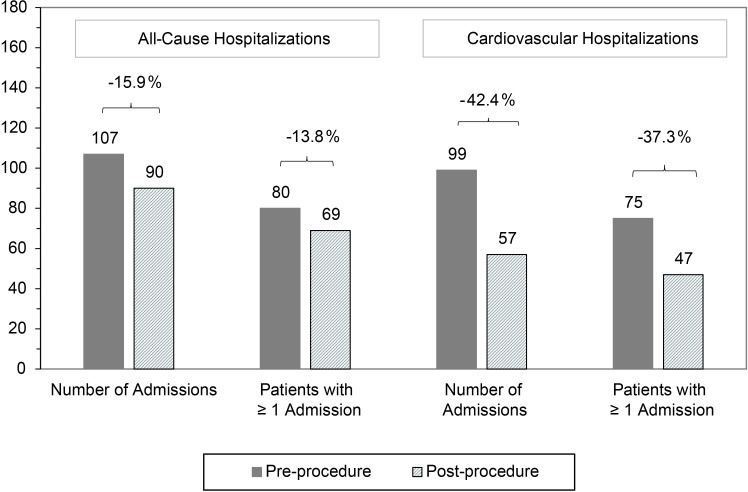
Results: Both QOL instruments showed significant 12-month improvements across all domains: AFEQT score increased 25.1-37.5 points and 33.3%-50.8% fewer patients reporting any problem across EuroQoL EQ-5D-5L domains. Overall, AFEQT improvement was highly associated with AF burden (p=0.009 for <10% vs ≥10% burden, p<0.001 for <20% vs ≥20% burden). Cardiovascular hospitalisations were significantly decreased after ablation (42%, p=0.001). Patients without substantial improvement in AFEQT (55/301, 18.2%) had higher AFEQT and CHA2DS2-VASc scores at baseline, and higher AF burden following PVI.
Conclusions: QOL improved and healthcare utilisation decreased significantly after ablation with a standardised CLOSE protocol. QOL improvement was significantly associated with impairment at baseline and AF burden after ablation.
Trial registration number: NCT03062046.
Keywords: atrial fibrillation; catheter ablation.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: Dr MD reports personal fees (consulting) from Biosense Webster, outside the submitted work; reports non-financial (travel) support for the submitted work. Dr RK reports grants from Biosense Webster, grants from Biotronik, grants from Abbott, grants from Medtronic, grants from Boston, grants from SIS Medical, outside the submitted work. Dr GS reports grants from Biosense Webster, during the conduct of the study; personal fees from Biosense Webster, personal fees from Abbott, outside the submitted work. Dr J-PA reports personal fees (consulting) from Biosense Webster and from Abbott outside the submitted work. Drs BB, TDP, SK, NS, DS, YS, PT, HVH, JV and MW have nothing to disclose.
Figures

References
-
- Phlips T, Taghji P, El Haddad M, et al. Improving procedural and one-year outcome after contact force-guided pulmonary vein isolation: the role of interlesion distance, ablation index, and contact force variability in the 'CLOSE'-protocol. Europace 2018;20:f419–27. 10.1093/europace/eux376 - DOI - PubMed
-
- Duytschaever M, Vijgen J, De Potter T, et al. Standardized pulmonary vein isolation workflow to enclose veins with contiguous lesions: the multicenter VISTAX trial. Europace. In Press 2020. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical