

Tumor-Associated Stromal Cellular Density as a Predictor of Recurrence and Mortality in Breast Cancer: Results from Ethnically Diverse Study Populations
- PMID: 33952648
- PMCID: PMC8254774
- DOI: 10.1158/1055-9965.EPI-21-0055
Tumor-Associated Stromal Cellular Density as a Predictor of Recurrence and Mortality in Breast Cancer: Results from Ethnically Diverse Study Populations
Abstract
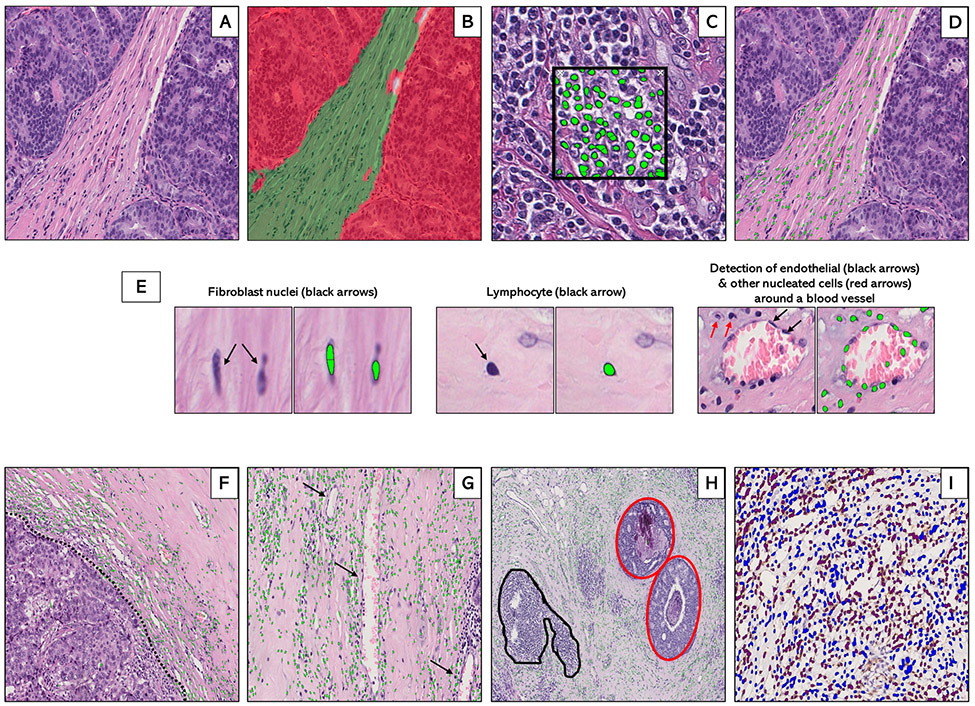
Purpose: Tumor-associated stroma is comprised of fibroblasts, tumor-infiltrating lymphocytes (TIL), macrophages, endothelial cells, and other cells that interactively influence tumor progression through inflammation and wound repair. Although gene-expression signatures reflecting wound repair predict breast cancer survival, it is unclear whether combined density of tumor-associated stromal cells, a morphologic proxy for inflammation and wound repair signatures on routine hematoxylin and eosin (H&E)-stained sections, is of prognostic relevance.
Methods: By applying machine learning to digitized H&E-stained sections for 2,084 breast cancer patients from China (n = 596; 24-55 years), Poland (n = 810; 31-75 years), and the United States (n = 678; 55-78 years), we characterized tumor-associated stromal cellular density (SCD) as the percentage of tumor-stroma that is occupied by nucleated cells. Hazard ratios (HR) and 95% confidence intervals (CI) for associations between SCD and clinical outcomes [recurrence (China) and mortality (Poland and the United States)] were estimated using Cox proportional hazard regression, adjusted for clinical variables.
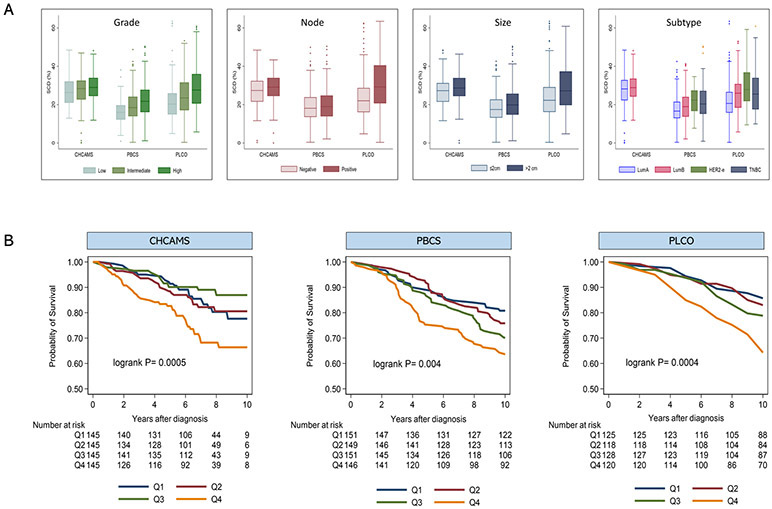
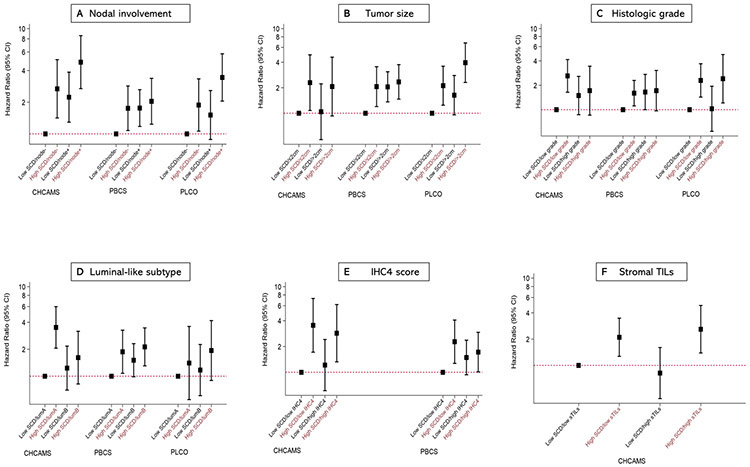
Results: SCD was independently predictive of poor clinical outcomes in hormone receptor-positive (luminal) tumors from China [multivariable HR (95% CI)fourth(Q4) vs. first(Q1) quartile = 1.86 (1.06-3.26); P trend = 0.03], Poland [HR (95% CI)Q4 vs. Q1 = 1.80 (1.12-2.89); P trend = 0.01], and the United States [HR (95% CI)Q4 vs. Q1 = 2.42 (1.33-4.42); P trend = 0.002]. In general, SCD provided more prognostic information than most classic clinicopathologic factors, including grade, size, PR, HER2, IHC4, and TILs, predicting clinical outcomes irrespective of menopausal or lymph nodal status. SCD was not predictive of outcomes in hormone receptor-negative tumors.
Conclusions: Our findings support the independent prognostic value of tumor-associated SCD among ethnically diverse luminal breast cancer patients.
Impact: Assessment of tumor-associated SCD on standard H&E could help refine prognostic assessment and therapeutic decision making in luminal breast cancer.
©2021 American Association for Cancer Research.
Conflict of interest statement
Disclosures of Potential Conflicts of Interest:
The authors declare no conflicts of interest
Figures
References
-
- Beck AH, Sangoi AR, Leung S, Marinelli RJ, Nielsen TO, van de Vijver MJ, et al. Systematic Analysis of Breast Cancer Morphology Uncovers Stromal Features Associated with Survival. Science Translational Medicine. 2011;3(108):108ra13–ra13. - PubMed
-
- Yuan Y, Failmezger H, Rueda OM, Ali HR, Gräf S, Chin S-F, et al. Quantitative Image Analysis of Cellular Heterogeneity in Breast Tumors Complements Genomic Profiling. Science Translational Medicine. 2012;4(157):157ra43–ra43. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
