

Clearance of Clostridioides difficile Colonization Is Associated with Antibiotic-Specific Bacterial Changes
- PMID: 33952668
- PMCID: PMC8103992
- DOI: 10.1128/mSphere.01238-20
Clearance of Clostridioides difficile Colonization Is Associated with Antibiotic-Specific Bacterial Changes
Abstract
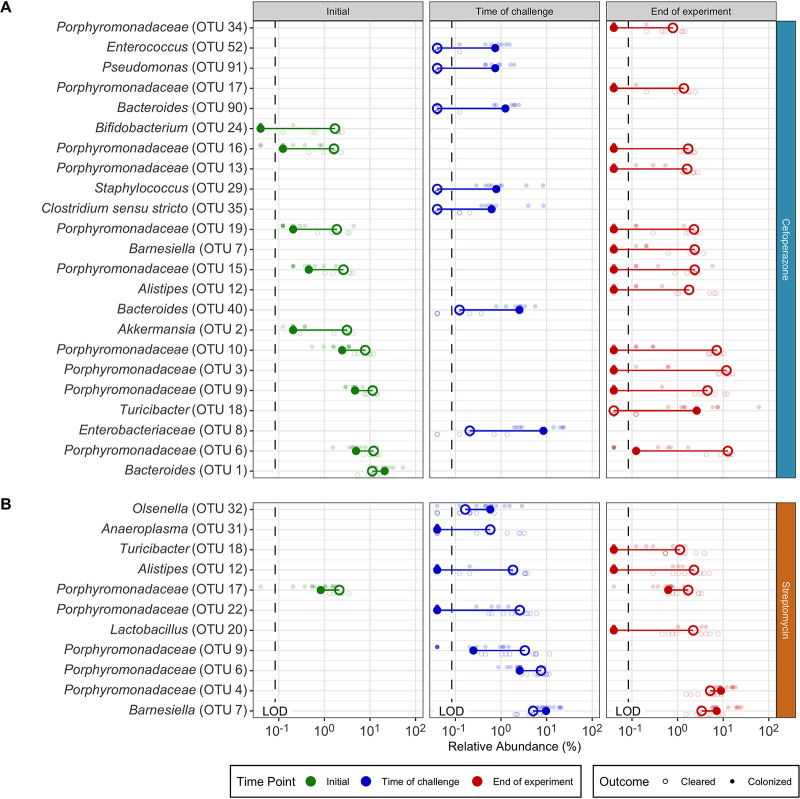
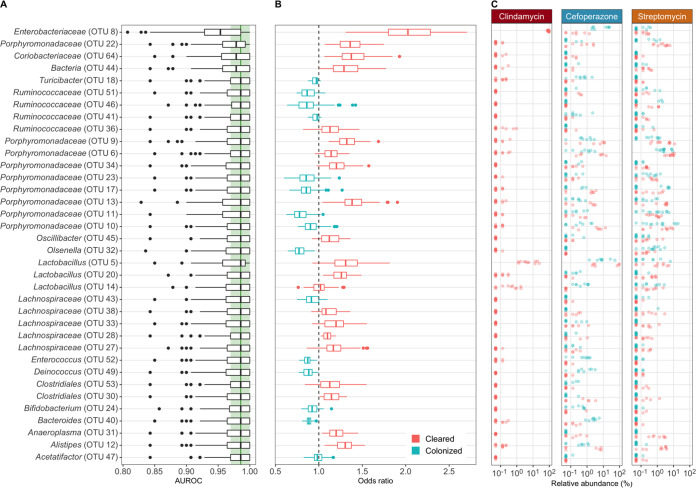
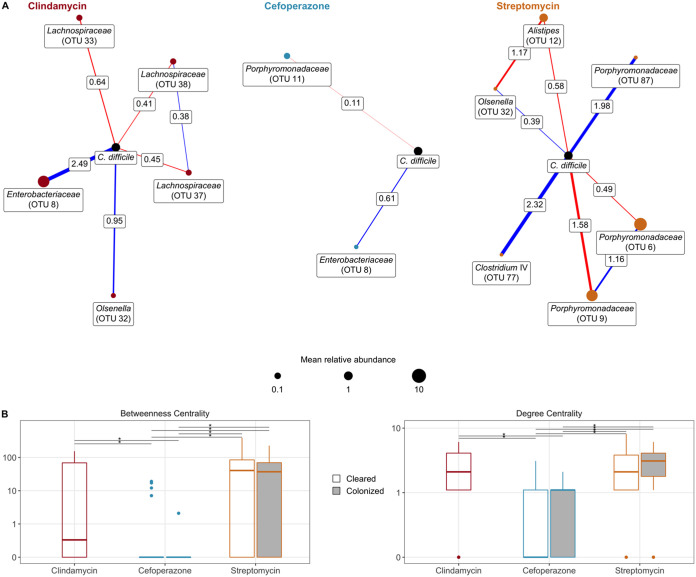
The gut bacterial community prevents many pathogens from colonizing the intestine. Previous studies have associated specific bacteria with clearing Clostridioides difficile colonization across different community perturbations. However, those bacteria alone have been unable to clear C. difficile colonization. To elucidate the changes necessary to clear colonization, we compared differences in bacterial abundance between communities able and unable to clear C. difficile colonization. We treated mice with titrated doses of antibiotics prior to C. difficile challenge, resulting in no colonization, colonization and clearance, or persistent colonization. Previously, we observed that clindamycin-treated mice were susceptible to colonization but spontaneously cleared C. difficile Therefore, we investigated whether other antibiotics would show the same result. We found that reduced doses of cefoperazone and streptomycin permitted colonization and clearance of C. difficile Mice that cleared colonization had antibiotic-specific community changes and predicted interactions with C. difficile Clindamycin treatment led to a bloom in populations related to Enterobacteriaceae Clearance of C. difficile was concurrent with the reduction of those blooming populations and the restoration of community members related to the Porphyromonadaceae and Bacteroides Cefoperazone created a susceptible community characterized by drastic reductions in the community diversity and interactions and a sustained increase in the abundance of many facultative anaerobes. Lastly, clearance in streptomycin-treated mice was associated with the recovery of multiple members of the Porphyromonadaceae, with little overlap in the specific Porphyromonadaceae observed in the clindamycin treatment. Further elucidation of how C. difficile colonization is cleared from different gut bacterial communities will improve C. difficile infection treatments.IMPORTANCE The community of microorganisms, or microbiota, in our intestines prevents pathogens like C. difficile from colonizing and causing infection. However, antibiotics can disturb the gut microbiota, which allows C. difficile to colonize. C. difficile infections (CDI) are primarily treated with antibiotics, which frequently leads to recurrent infections because the microbiota has not yet returned to a resistant state. The recurrent infection cycle often ends when the fecal microbiota from a presumed resistant person is transplanted into the susceptible person. Although this treatment is highly effective, we do not understand the mechanism. We hope to improve the treatment of CDI through elucidating how the bacterial community eliminates CDI. We found that C. difficile colonized susceptible mice but was spontaneously eliminated in an antibiotic treatment-specific manner. These data indicate that each community had different requirements for clearing colonization. Understanding how different communities clear colonization will reveal targets to improve CDI treatments.
Keywords: 16S rRNA gene; Clostridioides difficile; Clostridium difficile; colonization resistance; dynamics; microbial ecology; microbiome; microbiota.
Copyright © 2021 Lesniak et al.
Figures



References
-
- Lessa FC, Mu Y, Bamberg WM, Beldavs ZG, Dumyati GK, Dunn JR, Farley MM, Holzbauer SM, Meek JI, Phipps EC, Wilson LE, Winston LG, Cohen JA, Limbago BM, Fridkin SK, Gerding DN, McDonald LC. 2015. Burden of Clostridium difficile infection in the United States. N Engl J Med 372:825–834. doi:10.1056/NEJMoa1408913. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
