

Age-Related Clinical Outcomes of Patients with Non-Valvular Atrial Fibrillation: Insights from the COOL-AF Registry
- PMID: 33953549
- PMCID: PMC8089026
- DOI: 10.2147/CIA.S302389
Age-Related Clinical Outcomes of Patients with Non-Valvular Atrial Fibrillation: Insights from the COOL-AF Registry
Abstract
Purpose: We aimed to compare the rate of clinical outcomes among three age groups (<65, 65-74, and ≥75 years) of adult patients with non-valvular atrial fibrillation (NVAF).
Patients and methods: We prospectively enrolled NVAF patients from 27 Thailand medical centers. The following were collected at baseline: demographic data, risk factors, comorbid conditions, laboratory data, and medications. The clinical outcomes were ischemic stroke (IS) or transient ischemic attack (TIA), major bleeding (MB), intracerebral hemorrhage (ICH), heart failure (HF), and death. All events were adjudicated. Patients were categorized according to age group into three groups; age <65, 65-74, and ≥75 years.
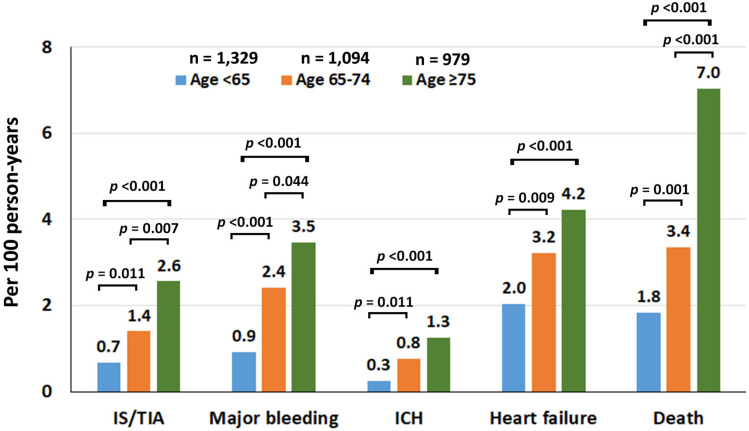
Results: Among the 3402 patients that were enrolled during 2014-2017, the mean age was 67.4±11.3 years, and 2073 (60.9%) were older. The average follow-up was 25.7±10.6 months. Oral anticoagulants were given in 75.4% of patients (91.1% of OAC was warfarin). The incidence rate of IS/TIA, MB, ICH, HF, and death was 1.43 (1.17-1.74), 2.11 (1.79-2.48), 0.70 (0.52-0.92), 3.03 (2.64-3.46), and 3.77 (3.33-4.24) per 100 person-years, respectively. The risk of IS/TIA, MB, ICH, HF, and death increased with age both before and after adjustment for potential confounders. Even though OAC reduced the risk of IS/TIA, it increased the risk of MB. Net clinical benefit (NCB) analysis favored oral anticoagulant (OAC) in the high-risk subset of older adults.
Conclusion: Older adult NVAF patients had a significantly increased risk of IS/TIA, MB, ICH, HF, and death compared to younger NVAF before and after adjustment for potential confounders. Strategies to reduce overall risk, including OAC use and choice and integrated care, should be implemented.
Keywords: COOL-AF registry; NVAF; Thailand; age-related clinical outcomes; non-valvular atrial fibrillation; patients.
© 2021 Krittayaphong et al.
Conflict of interest statement
All authors declare no conflicts of interest for this work and no financial support from the companies that produce and/or distribute the drugs, devices, or materials described in this report.
Figures




References
-
- Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37(38):2893–2962. - PubMed
-
- Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137(2):263–272. doi: 10.1378/chest.09-1584 - DOI - PubMed
-
- Krittayaphong R, Phrommintikul A, Ngamjanyaporn P, et al. Rate of anticoagulant use, and factors associated with not prescribing anticoagulant in older Thai adults with non-valvular atrial fibrillation: a multicenter registry. J Geriatr Cardiol. 2019;16(3):242–250. doi: 10.11909/j.issn.1671-5411.2019.03.004 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
