

Epicardial Adipose Tissue Volume Is Associated with High Risk Plaque Profiles in Suspect CAD Patients
- PMID: 33953836
- PMCID: PMC8057896
- DOI: 10.1155/2021/6663948
Epicardial Adipose Tissue Volume Is Associated with High Risk Plaque Profiles in Suspect CAD Patients
Retraction in
-
Retracted: Epicardial Adipose Tissue Volume Is Associated with High Risk Plaque Profiles in Suspect CAD Patients.Oxid Med Cell Longev. 2023 Oct 11;2023:9767518. doi: 10.1155/2023/9767518. eCollection 2023. Oxid Med Cell Longev. 2023. PMID: 37868734 Free PMC article.
Abstract
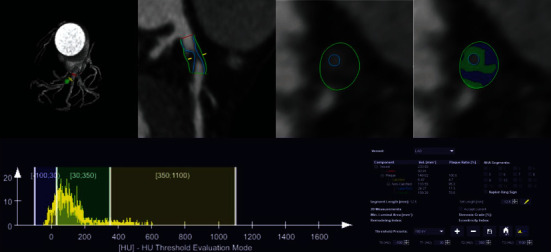
Objective: To explore the association between EAT volume and plaque precise composition and high risk plaque detected by coronary computed tomography angiography (CCTA).
Methods: 101 patients with suspected coronary artery disease (CAD) underwent CCTA examination from March to July 2019 were enrolled, including 70 cases acute coronary syndrome (ACS) and 31 cases stable angina pectoris (SAP). Based on CCTA image, atherosclerotic plaque precise compositions were analyzed using dedicated quantitative software. High risk plaque was defined as plaque with more than 2 high risk features (spotty calcium, positive remolding, low attenuation plaque, napkin-ring sign) on CCTA image. The association between EAT volume and plaque composition was assessed as well as the different of correlation between ACS and SAP was analyzed. Multivariable logistic regression analysis was used to explore whether EAT volume was independent risk factors of high risk plaque (HRP).
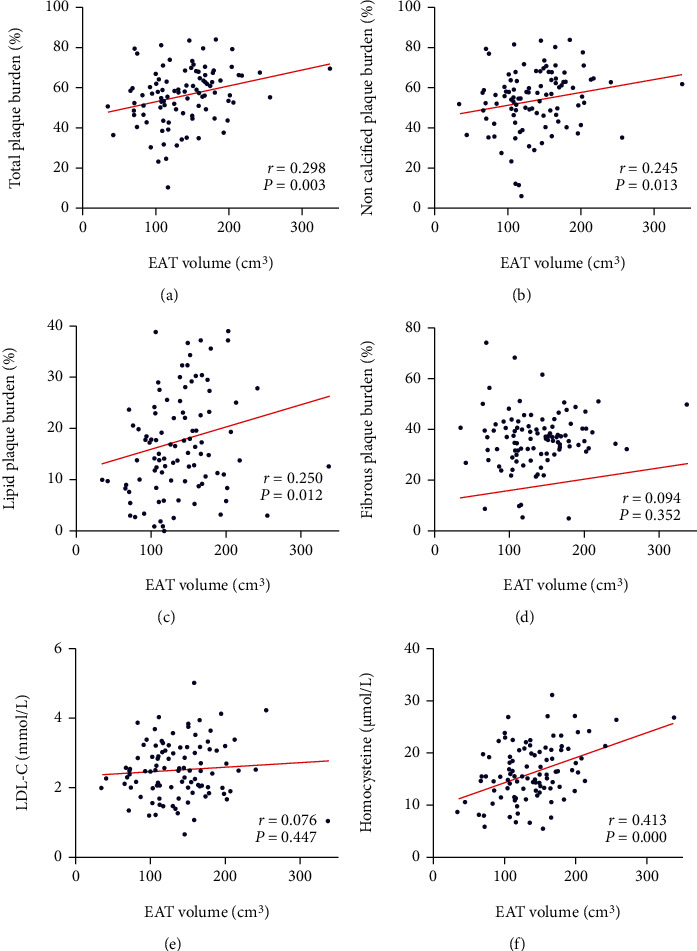
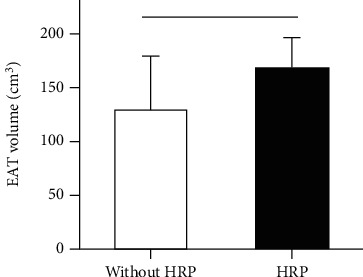
Results: EAT volume in the ACS group was significantly higher than that of the SAP group (143.7 ± 49.8 cm3 vs. 123.3 ± 39.2 cm3, P = 0.046). EAT volume demonstrated a significant positive correlation with total plaque burden (r = 0.298, P = 0.003), noncalcified plaque burden (r = 0.245, P = 0.013), lipid plaque burden (r = 0.250, P = 0.012), and homocysteine (r = 0.413, P ≤ 0.001). In ACS, EAT volume was positively correlated with total plaque burden (r = 0.309, P = 0.009), noncalcified plaque burden (r = 0.242, P = 0.044), and lipid plaque burden (r = 0.240, P = 0.045); however, no correlation was observed in SAP. Patients with HRP have larger EAT volume than those without HRP (169 ± 6.2 cm3 vs. 130.6 ± 5.3 cm3, P = 0.002). After adjustment by traditional risk factors and coronary artery calcium score (CACS), EAT volume was an independent risk predictor of presence of HRP (OR: 1.018 (95% CI: 1.006-1.030), P = 0.004).
Conclusions: With the increasing EAT volume, more dangerous plaque composition burdens increase significantly. EAT volume is a risk predictor of HRP independent of convention cardiovascular risk factors and CACS, which supports the potential impact of EAT on progression of coronary atherosclerotic plaque.
Copyright © 2021 Dongkai Shan et al.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Kitagawa T., Yamamoto H., Horiguchi J., et al. Characterization of noncalcified coronary plaques and identification of culprit lesions in patients with acute coronary syndrome by 64-slice computed tomography. JACC: Cardiovascular Imaging. 2009;2(2):153–160. doi: 10.1016/j.jcmg.2008.09.015. - DOI - PubMed
-
- Puchner S. B., Liu T., Mayrhofer T., et al. High-risk plaque detected on coronary CT angiography predicts acute coronary syndromes independent of significant stenosis in acute chest pain: results from the ROMICAT-II trial. Journal of the American College of Cardiology. 2014;64(7):684–692. doi: 10.1016/j.jacc.2014.05.039. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
