

Randomised controlled trial of oxygen therapy and high-flow nasal therapy in African children with pneumonia
- PMID: 33954839
- PMCID: PMC8098782
- DOI: 10.1007/s00134-021-06385-3
Randomised controlled trial of oxygen therapy and high-flow nasal therapy in African children with pneumonia
Abstract
Purpose: The life-saving role of oxygen therapy in African children with severe pneumonia is not yet established.
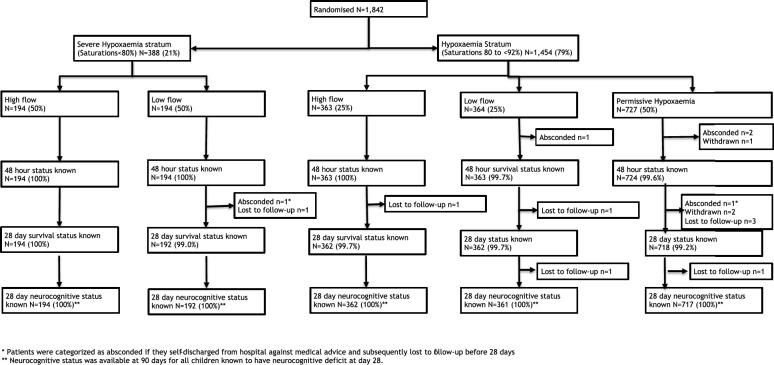
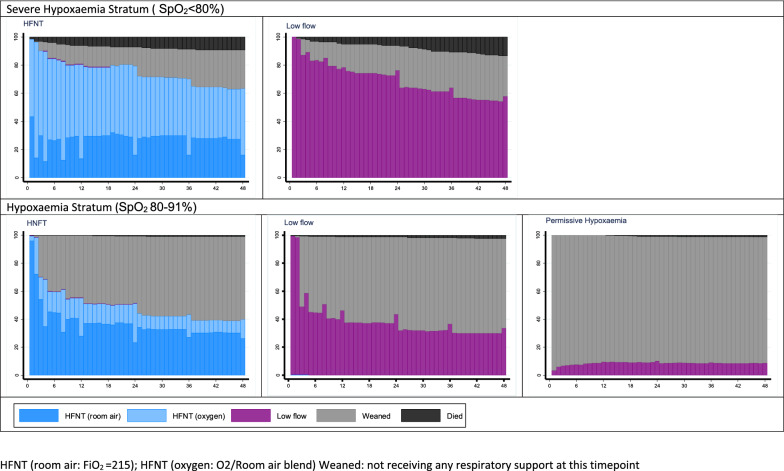
Methods: The open-label fractional-factorial COAST trial randomised eligible Ugandan and Kenyan children aged > 28 days with severe pneumonia and severe hypoxaemia stratum (SpO2 < 80%) to high-flow nasal therapy (HFNT) or low-flow oxygen (LFO: standard care) and hypoxaemia stratum (SpO2 80-91%) to HFNT or LFO (liberal strategies) or permissive hypoxaemia (ratio 1:1:2). Children with cyanotic heart disease, chronic lung disease or > 3 h receipt of oxygen were excluded. The primary endpoint was 48 h mortality; secondary endpoints included mortality or neurocognitive sequelae at 28 days.
Results: The trial was stopped early after enrolling 1852/4200 children, including 388 in the severe hypoxaemia stratum (median 7 months; median SpO2 75%) randomised to HFNT (n = 194) or LFO (n = 194) and 1454 in the hypoxaemia stratum (median 9 months; median SpO2 88%) randomised to HFNT (n = 363) vs LFO (n = 364) vs permissive hypoxaemia (n = 727). Per-protocol 15% of patients in the permissive hypoxaemia group received oxygen (when SpO2 < 80%). In the severe hypoxaemia stratum, 48-h mortality was 9.3% for HFNT vs. 13.4% for LFO groups. In the hypoxaemia stratum, 48-h mortality was 1.1% for HFNT vs. 2.5% LFO and 1.4% for permissive hypoxaemia. In the hypoxaemia stratum, adjusted odds ratio for 48-h mortality in liberal vs permissive comparison was 1.16 (0.49-2.74; p = 0.73); HFNT vs LFO comparison was 0.60 (0.33-1.06; p = 0.08). Strata-specific 28 day mortality rates were, respectively: 18.6, 23.4 and 3.3, 4.1, 3.9%. Neurocognitive sequelae were rare.
Conclusions: Respiratory support with HFNT showing potential benefit should prompt further trials.
Keywords: African children; Clinical trial; High-flow nasal therapy; Oxygen; Pneumonia.
Conflict of interest statement
All authors declare no conflicts of interest.
Figures
Comment in
-
A COASTal view: where prior beliefs and uncertainty collide.Intensive Care Med. 2021 May;47(5):591-593. doi: 10.1007/s00134-021-06406-1. Epub 2021 Apr 27. Intensive Care Med. 2021. PMID: 33904949 No abstract available.
References
-
- Liu L, Oza S, Hogan D, Chu Y, Perin J, Zhu J, Lawn JE, Cousens S, Mathers C, Black RE. Global, regional, and national causes of under-5 mortality in 2000–15: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet. 2016;388(10063):3027–3035. doi: 10.1016/S0140-6736(16)31593-8. - DOI - PMC - PubMed
-
- Hospital Care for Children. Guidelines for the management of common childhood illnesses. Second Edition. In. Geneva: World Health Organization; 2013. - PubMed
-
- Recommendations for management of common childhood conditions: evidence for technical update of pocket book recommendations. In. Geneva: World Health Organization; 2012. - PubMed
-
- Mwaniki MK, Nokes DJ, Ignas J, Munywoki P, Ngama M, Newton CR, Maitland K, Berkley JA. Emergency triage assessment for hypoxaemia in neonates and young children in a Kenyan hospital: an observational study. Bull World Health Organ. 2009;87(4):263–270. doi: 10.2471/BLT.07.049148. - DOI - PMC - PubMed
-
- English M, Gathara D, Mwinga S, Ayieko P, Opondo C, Aluvaala J, Kihuba E, Mwaniki P, Were F, Irimu G, Wasunna A, Mogoa W, Nyamai R. Adoption of recommended practices and basic technologies in a low-income setting. Arch Dis Child. 2014;99(5):452–456. doi: 10.1136/archdischild-2013-305561. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
