

Risk of COVID-19 in Rheumatoid Arthritis: A National Veterans Affairs Matched Cohort Study in At-Risk Individuals
- PMID: 33955209
- PMCID: PMC8239709
- DOI: 10.1002/art.41800
Risk of COVID-19 in Rheumatoid Arthritis: A National Veterans Affairs Matched Cohort Study in At-Risk Individuals
Abstract
Objective: Rheumatoid arthritis (RA) and its treatments are associated with an increased risk of infection, but it remains unclear whether these factors have an impact on the risk or severity of COVID-19. The present study was undertaken to assess the risk and severity of COVID-19 in a US Department of Veterans Affairs (VA) cohort of patients with RA and those without RA.
Methods: A matched cohort study using national VA data was conducted. Patients diagnosed as having RA were identified among nondeceased individuals who were active in the VA health care system as of January 1, 2020 and who had received care in a VA medical center in 2019; patients for whom no RA diagnostic code was indicated were matched to the RA patients (1:1) by age, sex, and VA site (non-RA controls). Patients diagnosed as having COVID-19 and those with severe COVID-19 (defined as requiring hospitalization or leading to death) were ascertained from a national VA COVID-19 surveillance database through December 10, 2020. Multivariable Cox models were used to compare the risk of COVID-19 and COVID-19 hospitalization or death between RA patients and non-RA controls, after adjusting for demographic characteristics, comorbidities, health care utilization and access, and county-level COVID-19 incidence rates.
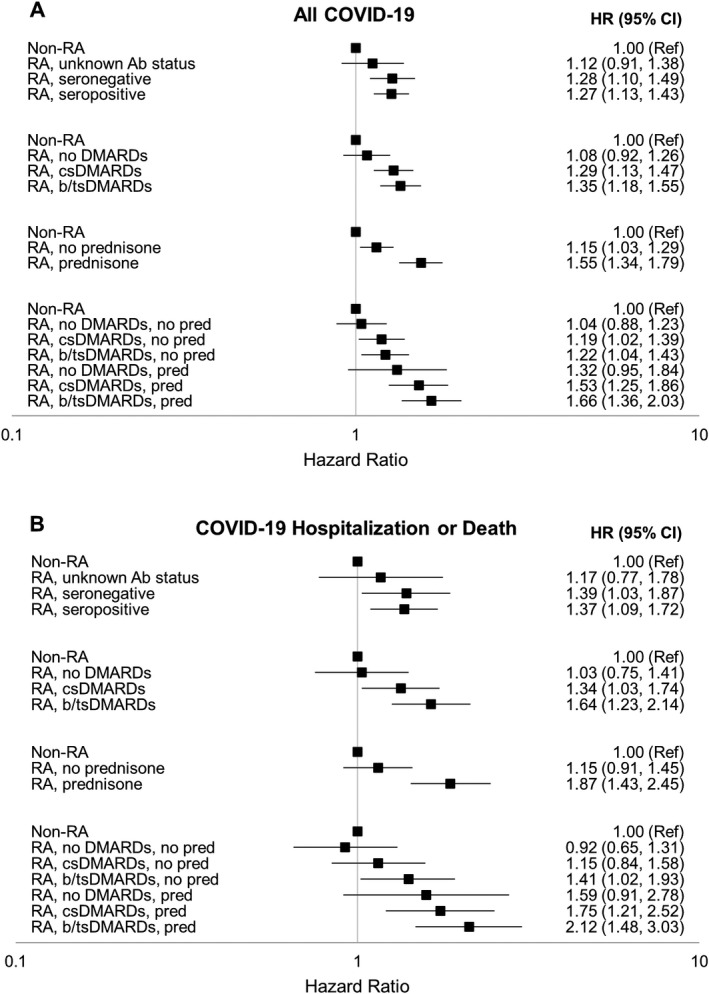
Results: This VA cohort of RA patients and non-RA controls (n = 33,886 subjects per group) predominantly comprised male patients (84.5%), and the mean age was 67.8 years. During follow-up, 1,503 patients in the cohort were diagnosed as having COVID-19; among them, 388 patients had severe COVID-19 (hospitalization or death), while in 228 patients, the deaths were not related to COVID-19. In the multivariable model, RA was associated with a higher risk of COVID-19 (adjusted hazard ratio [HR] 1.25 [95% confidence interval (95% CI) 1.13-1.39]) and a higher risk of COVID-19 hospitalization or death (adjusted HR 1.35 [95% CI 1.10-1.66]) as compared to non-RA controls. Use of disease-modifying antirheumatic drugs and prednisone, as well as self-reported Black race, self-reported Hispanic ethnicity, and presence of several chronic conditions, but not seropositivity for RA autoantibodies, were each associated with risk of COVID-19 and severe COVID-19 (hospitalization or death).
Conclusion: Patients with RA are at higher risk of developing COVID-19 and severe COVID-19 (leading to hospitalization or death) compared to those without RA. With a risk of COVID-19 that approaches that of other recognized chronic conditions, these findings suggest that RA patients should be prioritized for COVID-19 prevention and management strategies.
© 2021 American College of Rheumatology. This article has been contributed to by US Government employees and their work is in the public domain in the USA.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
