

Surgery for Bismuth-Corlette Type 4 Perihilar Cholangiocarcinoma: Results from a Western Multicenter Collaborative Group
- PMID: 33956275
- PMCID: PMC8519825
- DOI: 10.1245/s10434-021-09905-z
Surgery for Bismuth-Corlette Type 4 Perihilar Cholangiocarcinoma: Results from a Western Multicenter Collaborative Group
Abstract
Background: Although Bismuth-Corlette (BC) type 4 perihilar cholangiocarcinoma (pCCA) is no longer considered a contraindication for curative surgery, few data are available from Western series to indicate the outcomes for these patients. This study aimed to compare the short- and long-term outcomes for patients with BC type 4 versus BC types 2 and 3 pCCA undergoing surgical resection using a multi-institutional international database.
Methods: Uni- and multivariable analyses of patients undergoing surgery at 20 Western centers for BC types 2 and 3 pCCA and BC type 4 pCCA.
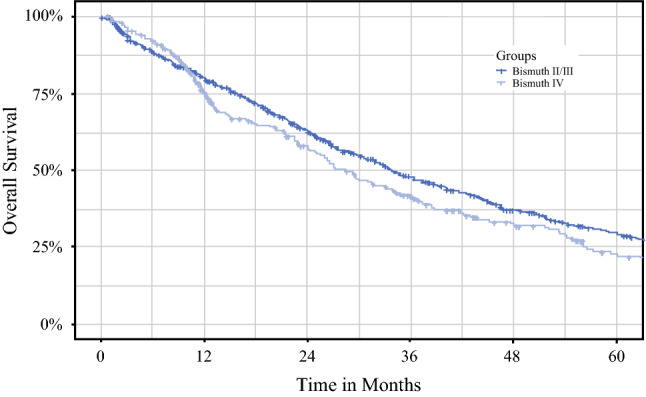
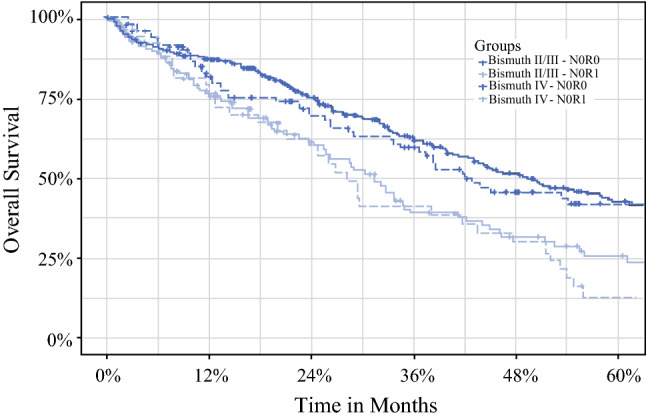
Results: Among 1138 pCCA patients included in the study, 826 (73%) had BC type 2 or 3 disease and 312 (27%) had type 4 disease. The two groups demonstrated significant differences in terms of clinicopathologic characteristics (i.e., portal vein embolization, extended hepatectomy, and positive margin). The incidence of severe complications was 46% for the BC types 2 and 3 patients and 51% for the BC type 4 patients (p = 0.1). Moreover, the 90-day mortality was 13% for the BC types 2 and 3 patients and 12% for the BC type 4 patients (p = 0.57). Lymph-node metastasis (N1; hazard-ratio [HR], 1.62), positive margins (R1; HR, 1.36), perineural invasion (HR, 1.53), and poor grade of differentiation (HR, 1.25) were predictors of survival (all p ≤0.004), but BC type was not associated with prognosis. Among the N0 and R0 patients, the 5-year overall survival was 43% for the patients with BC types 2 and 3 pCCA and 41% for those with BC type 4 pCCA (p = 0.60).
Conclusions: In this analysis of a large Western multi-institutional cohort, resection was shown to be an acceptable curative treatment option for selected patients with BC type 4 pCCA although a more technically challenging surgical approach was required.
© 2021. The Author(s).
Figures
Comment in
-
The Role of Surgery in the Treatment of Bismuth-Corlette Type IV Perihilar Cholangiocarcinoma.Ann Surg Oncol. 2021 Nov;28(12):7730. doi: 10.1245/s10434-021-09980-2. Epub 2021 Apr 21. Ann Surg Oncol. 2021. PMID: 33881654 No abstract available.
References
-
- Wiggers JK, Groot Koerkamp B, Cieslak KP, et al. Postoperative mortality after liver resection for perihilar cholangiocarcinoma: development of a risk score and importance of biliary drainage of the future liver remnant. J Am Coll Surg. 2016;223(2):321.e1–331.e1. doi: 10.1016/j.jamcollsurg.2016.03.035. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
