

Modelling optimal vaccination strategy for SARS-CoV-2 in the UK
- PMID: 33956791
- PMCID: PMC8101958
- DOI: 10.1371/journal.pcbi.1008849
Modelling optimal vaccination strategy for SARS-CoV-2 in the UK
Abstract
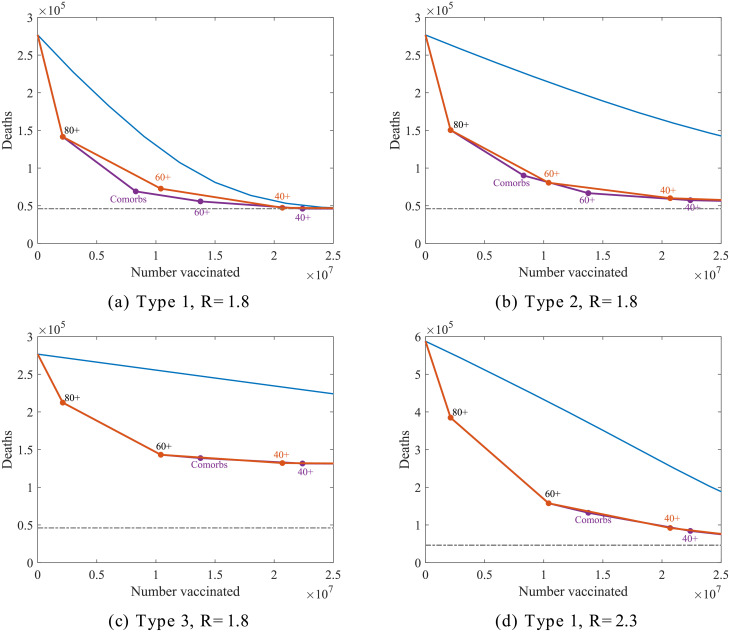
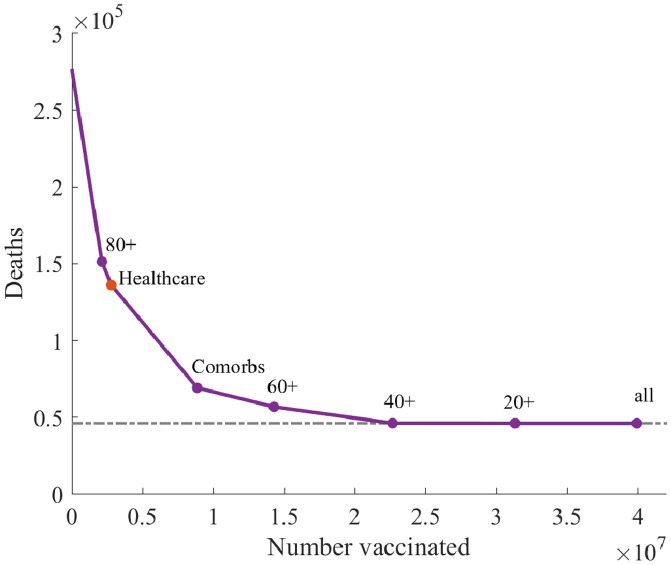
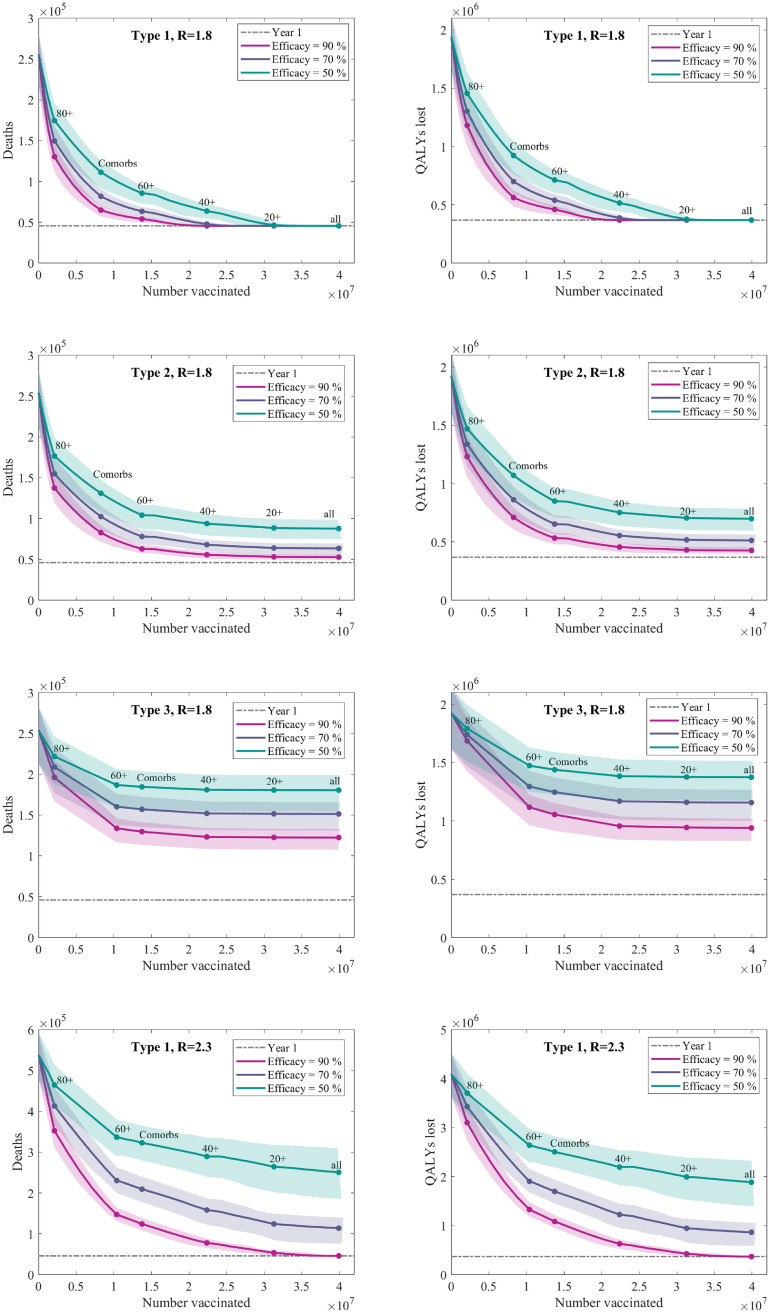
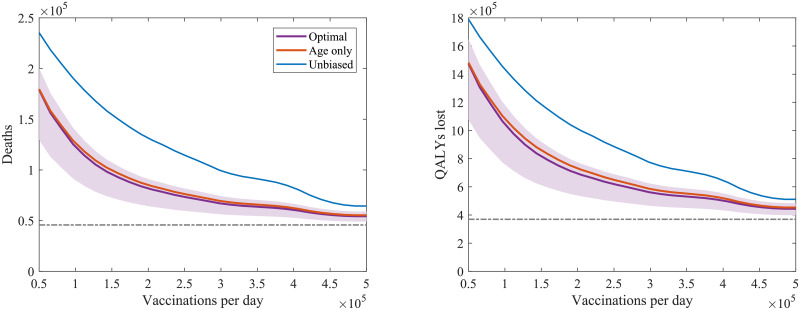
The COVID-19 outbreak has highlighted our vulnerability to novel infections. Faced with this threat and no effective treatment, in line with many other countries, the UK adopted enforced social distancing (lockdown) to reduce transmission-successfully reducing the reproductive number R below one. However, given the large pool of susceptible individuals that remain, complete relaxation of controls is likely to generate a substantial further outbreak. Vaccination remains the only foreseeable means of both containing the infection and returning to normal interactions and behaviour. Here, we consider the optimal targeting of vaccination within the UK, with the aim of minimising future deaths or quality adjusted life year (QALY) losses. We show that, for a range of assumptions on the action and efficacy of the vaccine, targeting older age groups first is optimal and may be sufficient to stem the epidemic if the vaccine prevents transmission as well as disease.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
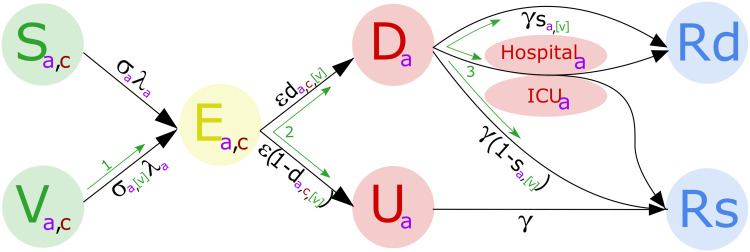
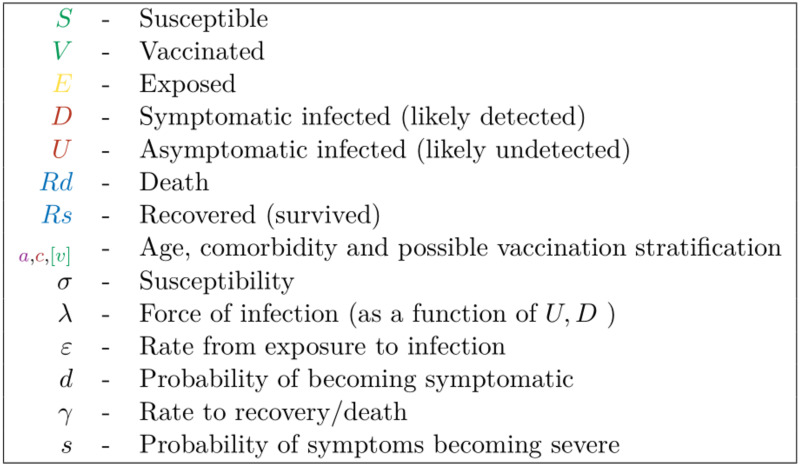
Reduction in susceptibility.
Reduction in becoming symptomatic.
Reduction in experiencing severe symptoms.
References
-
- Control for Disease Prevention EC. Covid-19 situation update worldwide, as of 16 august 2020. https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases (accessed August, 2020).
-
- NHS UK. Check if you or your child has coronavirus symptoms (2020). https://www.nhs.uk/conditions/coronavirus-covid-19/symptoms/. [Online] (Accessed: 11 December 2020).
-
- News B. Coronavirus vaccine: Uk government signs deals for 90 million doses. https://www.bbc.co.uk/news/health-53772650 (accessed August, 2020).
-
- Graham SP, McLean RK, Spencer AJ, Belij-Rammerstorfer S, Wright D, et al. Evaluation of the immunogenicity of prime-boost vaccination with the replication-deficient viral vectored covid-19 vaccine candidate chadox1 ncov-19. npj Vaccines 5(1):1–6 (2020). 10.1038/s41541-020-00221-3 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
