

Colonization With Fluoroquinolone-Resistant Enterobacterales Decreases the Effectiveness of Fluoroquinolone Prophylaxis in Hematopoietic Cell Transplant Recipients
- PMID: 33956965
- PMCID: PMC8492119
- DOI: 10.1093/cid/ciab404
Colonization With Fluoroquinolone-Resistant Enterobacterales Decreases the Effectiveness of Fluoroquinolone Prophylaxis in Hematopoietic Cell Transplant Recipients
Abstract
Background: Levofloxacin prophylaxis is recommended to prevent gram-negative bloodstream infections (BSIs) in patients with prolonged chemotherapy-induced neutropenia. However, increasing fluoroquinolone resistance may decrease the effectiveness of this approach.
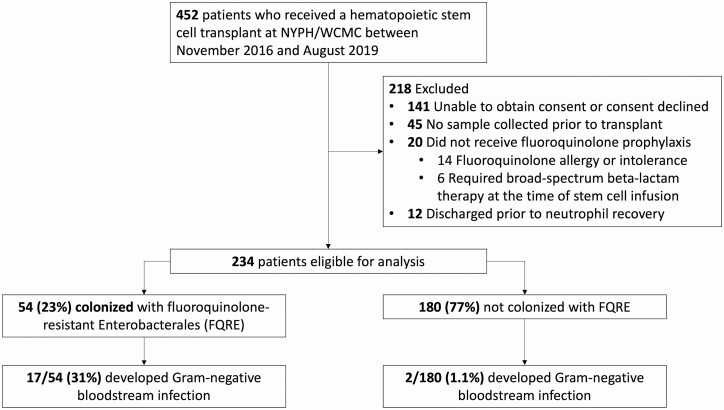
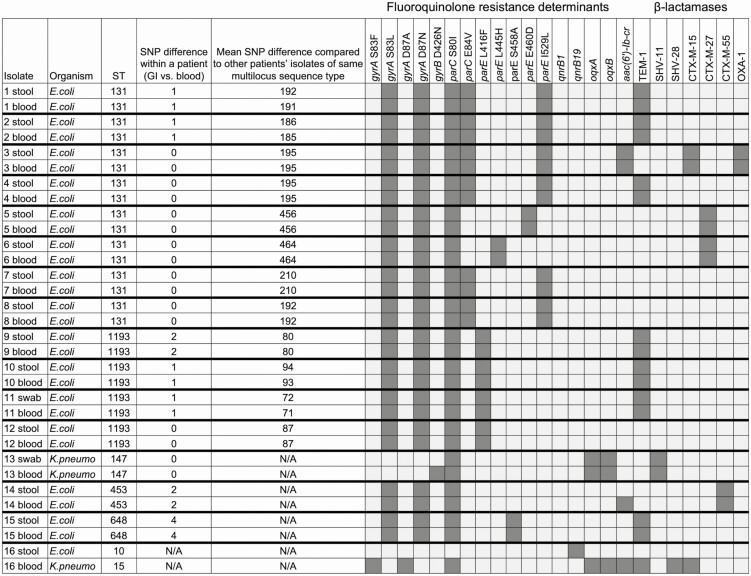
Methods: We assessed the prevalence of colonization with fluoroquinolone-resistant Enterobacterales (FQRE) among patients admitted for hematopoietic cell transplantation (HCT) from November 2016 to August 2019 and compared the risk of gram-negative BSI between FQRE-colonized and noncolonized patients. All patients received levofloxacin prophylaxis during neutropenia. Stool samples were collected upon admission for HCT and weekly thereafter until recovery from neutropenia, and underwent selective culture for FQRE. All isolates were identified and underwent antimicrobial susceptibility testing by broth microdilution. FQRE isolates also underwent whole-genome sequencing.
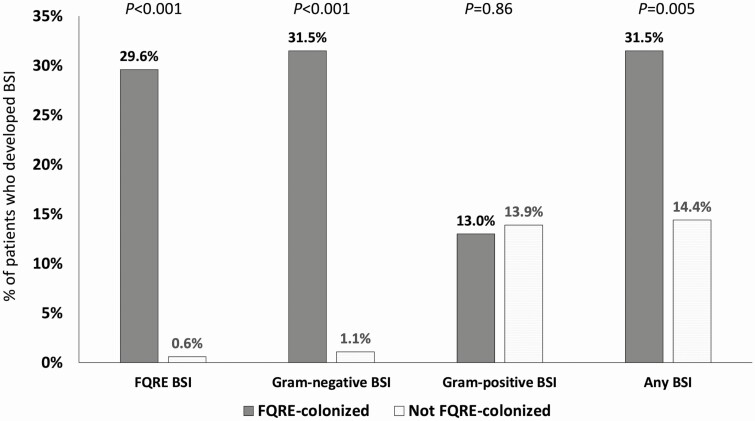
Results: Fifty-four of 234 (23%) patients were colonized with FQRE prior to HCT, including 30 of 119 (25%) allogeneic and 24 of 115 (21%) autologous HCT recipients. Recent antibacterial use was associated with FQRE colonization (P = .048). Ninety-one percent of colonizing FQRE isolates were Escherichia coli and 29% produced extended-spectrum β-lactamases. Seventeen (31%) FQRE-colonized patients developed gram-negative BSI despite levofloxacin prophylaxis, compared to only 2 of 180 (1.1%) patients who were not colonized with FQRE on admission (P < .001). Of the 17 gram-negative BSIs in FQRE-colonized patients, 15 (88%) were caused by FQRE isolates that were genetically identical to the colonizing strain.
Conclusions: Nearly one-third of HCT recipients with pretransplant FQRE colonization developed gram-negative BSI while receiving levofloxacin prophylaxis, and infections were typically caused by their colonizing strains. In contrast, levofloxacin prophylaxis was highly effective in patients not initially colonized with FQRE.
Keywords: fluoroquinolone resistance; hematopoietic cell transplant recipient; levofloxacin prophylaxis; neutropenia.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Can a Simple Stool Swab Predict Bacteremia in High-Risk Hematopoietic Cell Transplant Recipients?Clin Infect Dis. 2021 Oct 5;73(7):1266-1267. doi: 10.1093/cid/ciab412. Clin Infect Dis. 2021. PMID: 33961692 Free PMC article. No abstract available.
-
Cessation of Ciprofloxacin Prophylaxis in Hemato-Oncology Patients.Clin Infect Dis. 2022 Aug 24;75(1):178-179. doi: 10.1093/cid/ciab1000. Clin Infect Dis. 2022. PMID: 34864924 Free PMC article. No abstract available.
References
-
- Freifeld AG, Bow EJ, Sepkowitz KA, et al. ; Infectious Diseases Society of America. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the Infectious Diseases Society of America. Clin Infect Dis 2011; 52:427–31. - PubMed
-
- Taplitz RA, Kennedy EB, Bow EJ, et al. Antimicrobial prophylaxis for adult patients with cancer-related immunosuppression: ASCO and IDSA clinical practice guideline update. J Clin Oncol 2018; 36:3043–54. - PubMed
-
- Klastersky J, Ameye L, Maertens J, et al. Bacteraemia in febrile neutropenic cancer patients. Int J Antimicrob Agents 2007; 30(Suppl 1):S51–9. - PubMed
-
- Gudiol C, Bodro M, Simonetti A, et al. Changing aetiology, clinical features, antimicrobial resistance, and outcomes of bloodstream infection in neutropenic cancer patients. Clin Microbiol Infect 2013; 19:474–9. - PubMed
-
- Girmenia C, Bertaina A, Piciocchi A, et al. ; Gruppo Italiano Trapianto di Midollo Osseo (GITMO) and Associazione Microbiologi Clinici Italiani (AMCLI) . Incidence, risk factors and outcomes of pre-engraftment gram-negative bacteremia after allogeneic and autologous hematopoietic stem cell transplantation: an Italian prospective multicenter survey. Clin Infect Dis 2017; 65:1884–96. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
