

Defining Voiding Dysfunction in Women: Bladder Outflow Obstruction Versus Detrusor Underactivity
- PMID: 33957716
- PMCID: PMC8497729
- DOI: 10.5213/inj.2040342.171
Defining Voiding Dysfunction in Women: Bladder Outflow Obstruction Versus Detrusor Underactivity
Abstract
Purpose: We aimed to develop urodynamic criteria to improve the accuracy of the diagnosis of bladder outlet obstruction (BOO) and detrusor underactivity (DU) in women with lower urinary tract symptoms (LUTS).
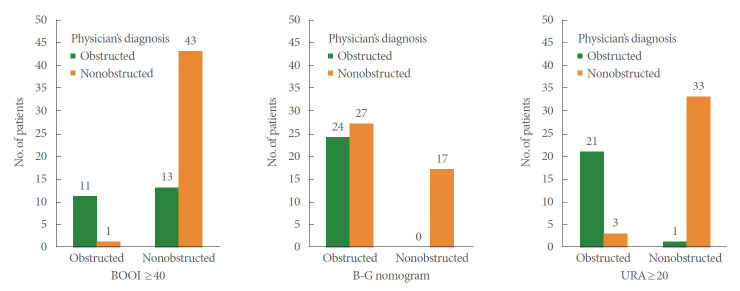
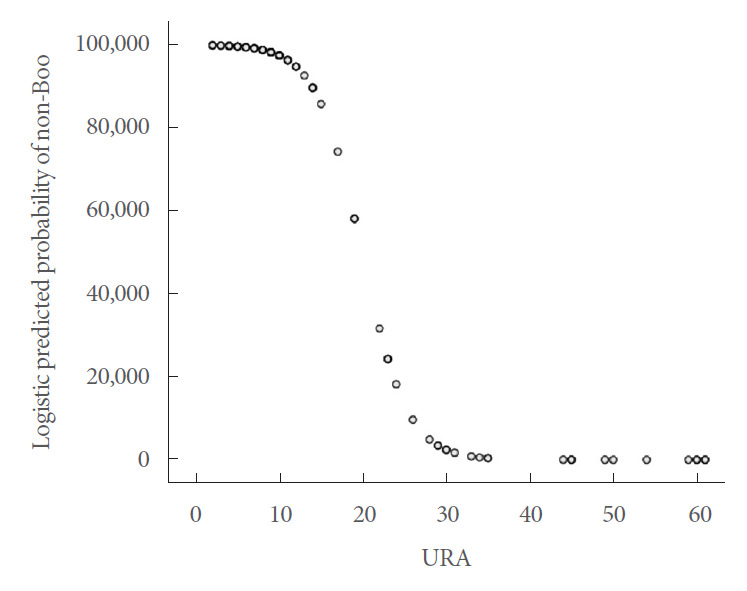
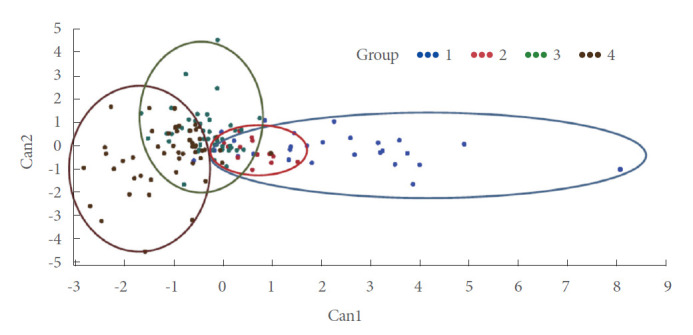
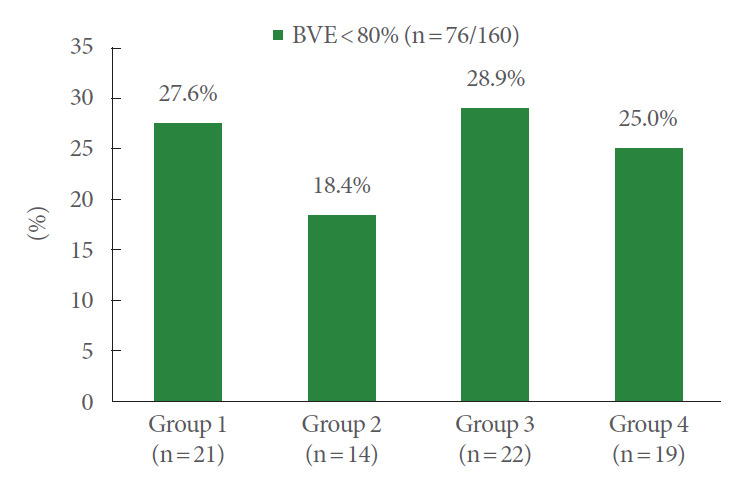
Methods: Initially, in a group of 68 consecutive women with LUTS and increased postvoid residual (PVR) who had undergone urodynamic investigations, we examined the level of agreement between the operating physician's diagnosis of BOO or DU and the diagnosis according to urodynamic nomograms/indices, including the Blaivas-Groutz (B-G) nomogram, urethral resistance factor (URA), bladder outlet obstruction index (BOOI), and bladder contractility index (BCI). Based on the initial results, we categorized 160 women into 4 groups using the B-G nomogram and URA (group 1, severe-moderate BOO; group 2, mild BOO and URA≥20; group 3, mild BOO and URA<20; group 4, nonobstructed) and compared the urodynamic parameters. Finally, we redefined women as obstructed (groups 1+2) and nonobstructed (groups 3+4) for subanalysis.
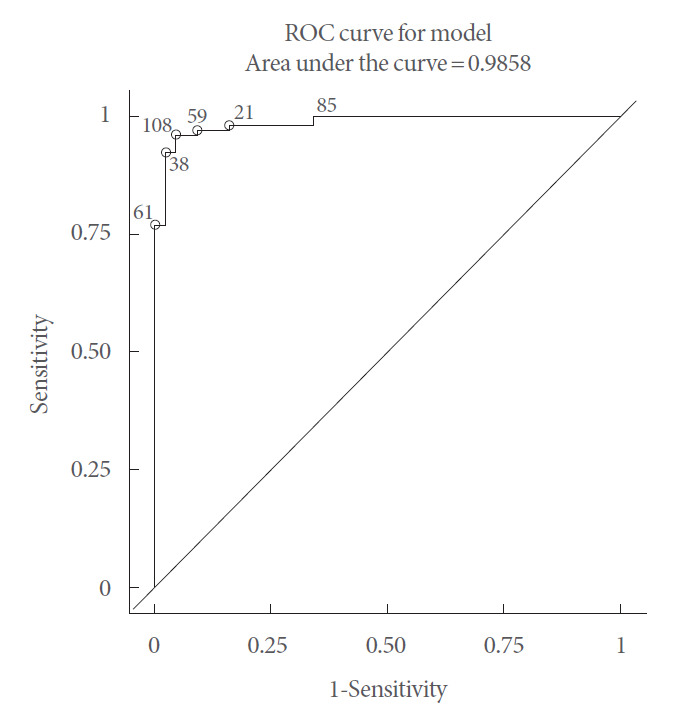
Results: The agreement between the B-G nomogram and physician's diagnosis was poor in the mild obstruction zone (κ=0.308, P=0.01). By adding URA (cutoff value=20), excellent agreement was reached (κ=0.856, P<0.001). Statistically significant differences were found among the 4 groups (analysis of variance) in maximum flow rate (Qmax) (P<0.0001), voided volume (VV) (P=0.042), PVR (P=0.032), BOOI (P<0.0001), and BCI (P<0.0001), with a positive linear trend for Qmax and VV and a negative linear trend for PVR and BOOI moving from groups 1 to 4. In the subanalysis, all parameters showed statistically significant differences between obstructed and nonobstructed women, except BCI (Qmax, P=0.0001; VV, P=0.0091; PVR, P=0.0005; BOOI, P=0.0001).
Conclusion: The combination of the B-G nomogram with URA increased the accuracy of diagnosing BOO among women with LUTS. Based on this combination, most women in the mild obstruction zone of the B-G nomogram would be considered underactive rather than obstructed.
Keywords: Lower urinary tract symptoms; Underactive; Urinary bladder; Urinary bladder neck obstruction.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Haylen BT, De Ridder D, Freeman RM, Swift SE, Berghmans B, Lee J, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urody. 2010;29:4–20. - PubMed
-
- Osman NI, Chapple CR, Abrams P, Dmochowski R, Haab F, Nitti V, et al. Detrusor underactivity and the underactive bladder: a new clinical entity? A review of current terminology, definitions, epidemiology, aetiology, and diagnosis. Eur Urol. 2014;65:389–98. - PubMed
-
- Sekido N. Bladder contractility and urethral resistance relation: what does a pressure flow study tell us? Int J Urol. 2012;19:216–28. - PubMed
-
- Groutz A, Blaivas JG. Non-neurogenic female voiding dysfunction. Curr Opin Urol. 2002;12:311–6. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
