

Progesterone levels on the human chorionic gonadotropin trigger day affect the pregnancy rates for embryos transferred at different stages of development in both general and selected IVF/ICSI populations
- PMID: 33957886
- PMCID: PMC8101180
- DOI: 10.1186/s12884-021-03832-3
Progesterone levels on the human chorionic gonadotropin trigger day affect the pregnancy rates for embryos transferred at different stages of development in both general and selected IVF/ICSI populations
Abstract
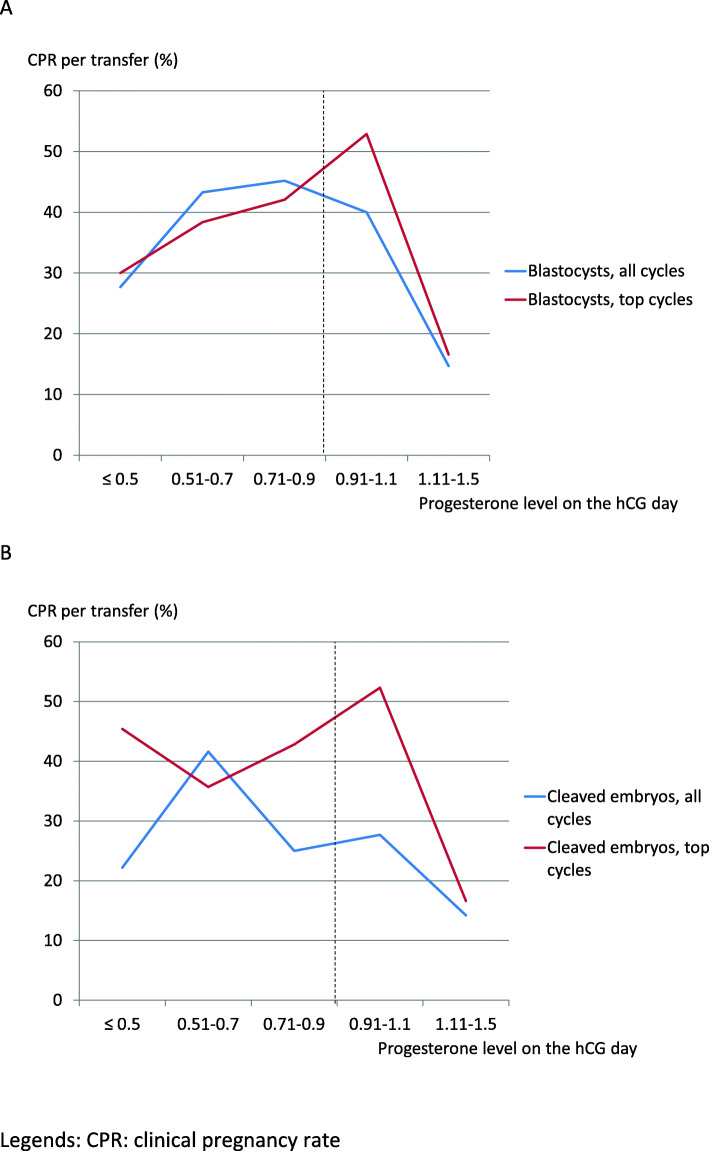
Background: Two meta-analyses have shown that pregnancy and birth rates are significantly higher after blastocyst transfer than after cleaved embryo transfer. Other studies have revealed that a serum progesterone level > 1.5 ng/ml on the trigger day is responsible for premature luteinization and is associated with a low pregnancy rate. The objectives of this retrospective study were to determine whether blastocyst transfer gave higher pregnancy rates than cleaved embryo transfer at day 3 in both the general and selected IVF/ICSI populations, and whether the serum progesterone level influenced the pregnancy rate.
Method: We studied IVF/ICSI cycles with GnRH antagonist - FSH/hMG protocols in a general population (n = 1210) and a selected "top cycle" population (n = 677), after blastocyst transfer on day 5 or cleaved embryo transfer on day 3. The selected couples had to meet the following criteria: female age < 35, first or second cycle, and one or two embryos transferred. We recorded predictive factors for pregnancy and calculated the progesterone to oocyte index (POI), the progesterone:estradiol ratio (P:E2 ratio), and the progesterone to follicle (> 14 mm) index (PFI).
Results: In the general population, the clinical pregnancy rate was significantly higher after blastocyst transfer (33.3%) than after cleaved embryo transfer (25.3%; p < 0.01); the same was true for the birth rate (32.1 and 22.8%, respectively, p < 0.01). The differences between blastocyst and embryo transfer groups were not significant in the selected population (respectively 35.7% vs. 35.8% for the clinical pregnancy rate, and 33.9 and 34.9% for the birth rate). The serum progesterone levels on the eve of the trigger day and on the day itself were significantly lower in the pregnant women (p < 0.01). We found a serum progesterone threshold of 0.9 ng/ml, as also reported by other researchers. The POI and the PFI appear to have predictive value for cleaved embryos transfers.
Conclusions: Blastocyst transfers were associated with higher clinical pregnancy and birth rates than cleaved embryo transfers in a general population but not in a selected population. The serum progesterone levels on the eve of the trigger day and on the day itself predicted the likelihood of pregnancy.
Keywords: Blastocyst; Cleaved embryo; IVF/ICSI; Pregnancy; Progesterone.
Conflict of interest statement
The authors report no conflicts of interest in relation to the present study.
Figures


References
-
- De Geyter C. More than 8 million babies born from IVF since the Worlof s first in 1978. 2018.
-
- Baker VL, Luke B, Brown MB, Alvero R, Frattarelli JL, Usadi R, et al. Multivariate analysis of factors affecting probability of pregnancy and live birth with in vitro fertilization: an analysis of the Society for Assisted Reproductive Technology Clinic Outcomes Reporting System. Fertil Steril. 2010;94:1410–1416. doi: 10.1016/j.fertnstert.2009.07.986. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
