

A nomogram for individualized prediction of overall survival in patients with newly diagnosed glioblastoma: a real-world retrospective cohort study
- PMID: 33957923
- PMCID: PMC8101102
- DOI: 10.1186/s12893-021-01233-z
A nomogram for individualized prediction of overall survival in patients with newly diagnosed glioblastoma: a real-world retrospective cohort study
Abstract
Background: This study aimed to identify the most valuable predictors of prognosis in glioblastoma (GBM) patients and develop and validate a nomogram to estimate individualized survival probability.
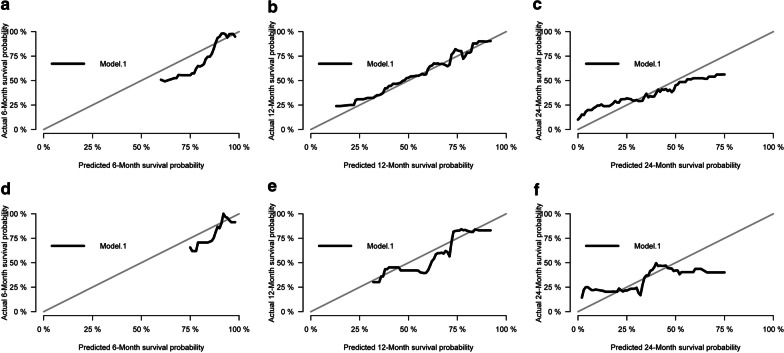
Methods: We conducted a real-world retrospective cohort study of 987 GBM patients diagnosed between September 2010 and December 2018. Computer generated random numbers were used to assign patients into a training cohort (694 patients) and internal validation cohort (293 patients). A least absolute shrinkage and selection operator (LASSO)-Cox model was used to select candidate variables for the prediction model. Cox proportional hazards regression was used to estimate overall survival. Models were internally validated using the bootstrap method and generated individualized predicted survival probabilities at 6, 12, and 24 months, which were compared with actual survival.
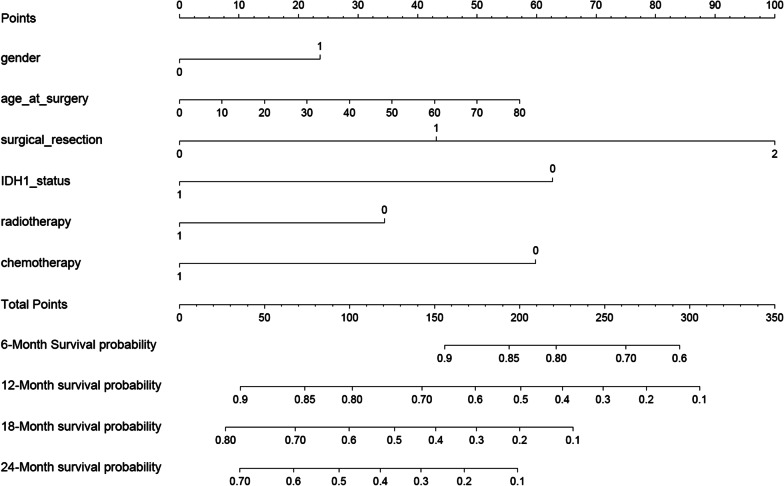
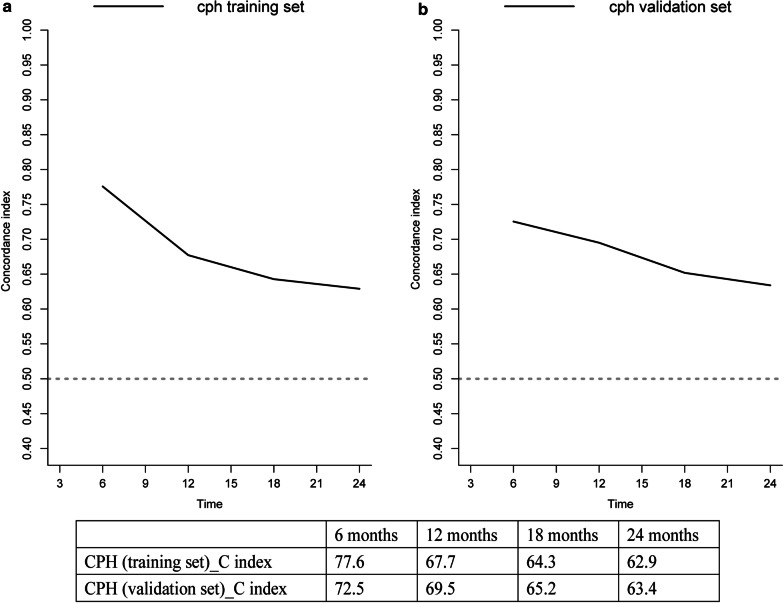
Results: The final nomogram was developed using the Cox proportional hazards model, which was the model with best fit and calibration. Gender, age at surgery, extent of tumor resection, radiotherapy, chemotherapy, and IDH1 mutation status were used as variables. The concordance indices for 6-, 12-, 18-, and 24-month survival probabilities were 0.776, 0.677, 0.643, and 0.629 in the training set, and 0.725, 0.695, 0.652, and 0.634 in the validation set, respectively.
Conclusions: Our nomogram that assesses individualized survival probabilities (6-, 12-, and 24-month) in newly diagnosed GBM patients can assist healthcare providers in optimizing treatment and counseling patients.
Trial registration: retrospectively registered.
Keywords: Glioblastoma; Lasso-Cox regression; Nomogram; Prognosis.
Conflict of interest statement
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Figures

Similar articles
-
An independently validated nomogram for individualized estimation of survival among patients with newly diagnosed glioblastoma: NRG Oncology RTOG 0525 and 0825.Neuro Oncol. 2017 May 1;19(5):669-677. doi: 10.1093/neuonc/now208. Neuro Oncol. 2017. PMID: 28453749 Free PMC article.
-
Validation and optimization of a web-based nomogram for predicting survival of patients with newly diagnosed glioblastoma.Strahlenther Onkol. 2020 Jan;196(1):58-69. doi: 10.1007/s00066-019-01512-y. Epub 2019 Sep 5. Strahlenther Onkol. 2020. PMID: 31489457 English.
-
An independently validated nomogram for isocitrate dehydrogenase-wild-type glioblastoma patient survival.Neurooncol Adv. 2019 May-Dec;1(1):vdz007. doi: 10.1093/noajnl/vdz007. Epub 2019 May 30. Neurooncol Adv. 2019. PMID: 31608326 Free PMC article.
-
Independently validated sex-specific nomograms for predicting survival in patients with newly diagnosed glioblastoma: NRG Oncology RTOG 0525 and 0825.J Neurooncol. 2021 Dec;155(3):363-372. doi: 10.1007/s11060-021-03886-5. Epub 2021 Nov 10. J Neurooncol. 2021. PMID: 34761331 Free PMC article.
-
Nomograms for prognostic risk assessment in glioblastoma multiforme: Applications and limitations.Clin Genet. 2022 Nov;102(5):359-368. doi: 10.1111/cge.14200. Epub 2022 Aug 1. Clin Genet. 2022. PMID: 35882630 Review.
Cited by
-
Small Molecule Immunomodulators as Next-Generation Therapeutics for Glioblastoma.Cancers (Basel). 2024 Jan 19;16(2):435. doi: 10.3390/cancers16020435. Cancers (Basel). 2024. PMID: 38275876 Free PMC article. Review.
-
Prediction of prognosis in glioblastoma with radiomics features extracted by synthetic MRI images using cycle-consistent GAN.Phys Eng Sci Med. 2024 Sep;47(3):1227-1243. doi: 10.1007/s13246-024-01443-8. Epub 2024 Jun 17. Phys Eng Sci Med. 2024. PMID: 38884673 Free PMC article.
-
Potential of Novel Methyl Jasmonate Analogs as Anticancer Agents to Metabolically Target HK-2 Activity in Glioblastoma Cells.Front Pharmacol. 2022 May 23;13:828400. doi: 10.3389/fphar.2022.828400. eCollection 2022. Front Pharmacol. 2022. PMID: 35677429 Free PMC article.
-
Systematic Review of Pre-Clinical Systems Using Artificial Microenvironments and Anti-Migratory Drugs to Control Migration of Glioblastoma Cells.Expert Rev Mol Med. 2025 Jan 23;27:e6. doi: 10.1017/erm.2024.33. Expert Rev Mol Med. 2025. PMID: 39844377 Free PMC article.
-
A 3-miRNA Signature Enables Risk Stratification in Glioblastoma Multiforme Patients with Different Clinical Outcomes.Curr Oncol. 2022 Jun 16;29(6):4315-4331. doi: 10.3390/curroncol29060345. Curr Oncol. 2022. PMID: 35735454 Free PMC article.
References
-
- Stupp R, Hegi ME, Mason WP, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–466. doi: 10.1016/S1470-2045(09)70025-7. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
