

Carotid endarterectomy with patch angioplasty versus primary closure in patients with symptomatic and significant stenosis: a systematic review with meta-analyses and trial sequential analysis of randomized clinical trials
- PMID: 33957978
- PMCID: PMC8103619
- DOI: 10.1186/s13643-021-01692-8
Carotid endarterectomy with patch angioplasty versus primary closure in patients with symptomatic and significant stenosis: a systematic review with meta-analyses and trial sequential analysis of randomized clinical trials
Abstract
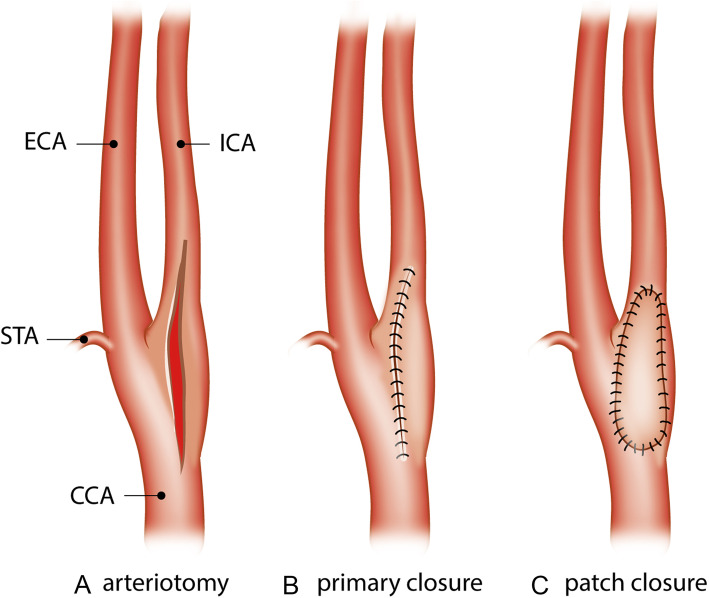
Background: Patch angioplasty in conventional carotid endarterectomy is suggested to reduce the risk of restenosis and recurrent ipsilateral stroke compared with primary closure. A systematic review of randomized clinical trials is needed to compare outcomes (benefits and harms) of both techniques.
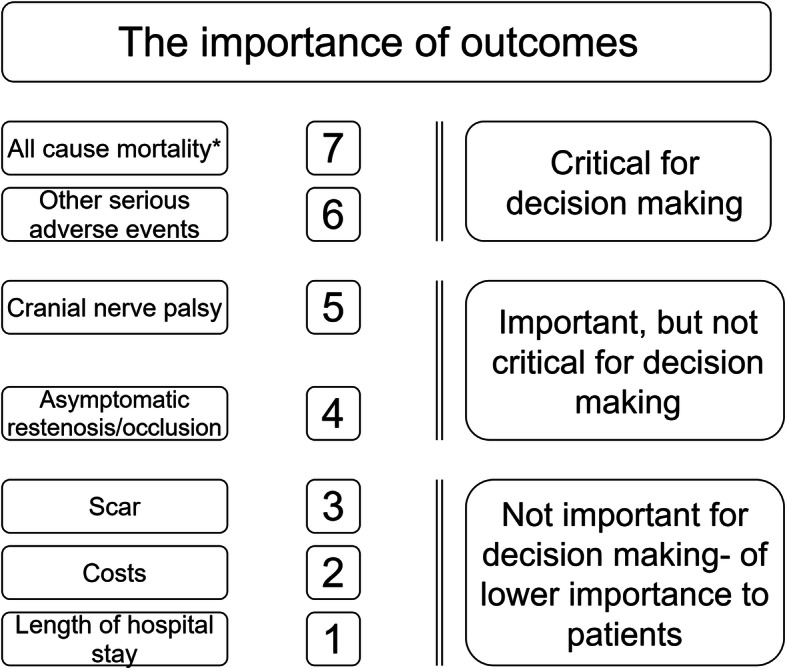
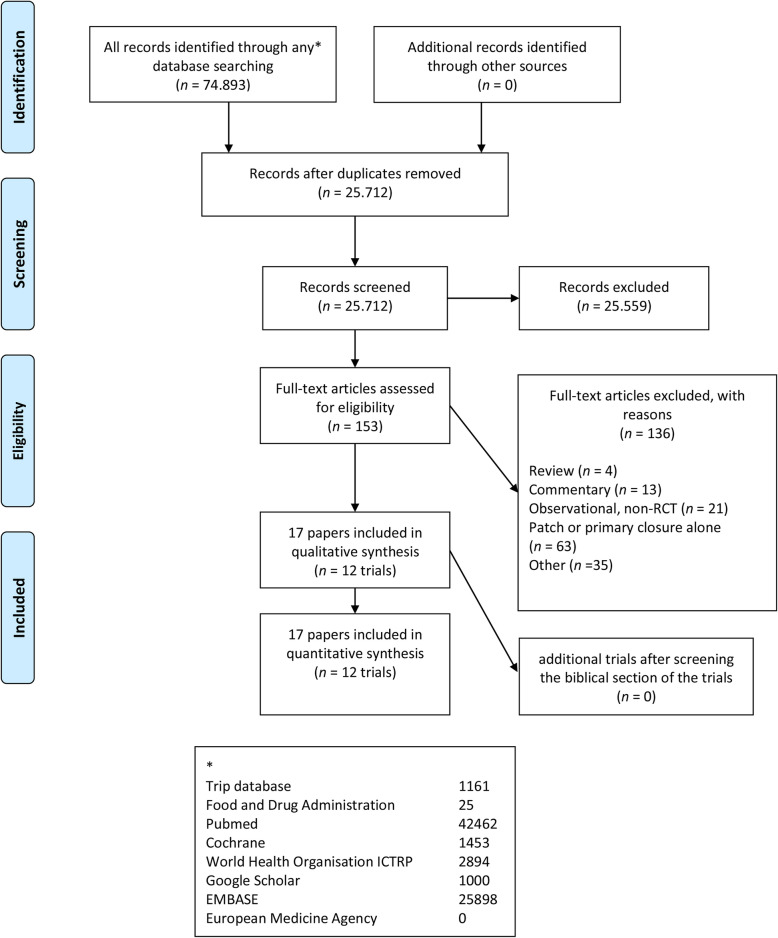
Methods: Searches (CENTRAL, PubMed/MEDLINE, EMBASE, and other databases) were last updated 3rd of January 2021. We included randomized clinical trials comparing carotid endarterectomy with patch angioplasty versus primary closure of the arterial wall in patients with a symptomatic and significant (> 50%) carotid stenosis. Primary outcomes are defined as all-cause mortality and serious adverse events.
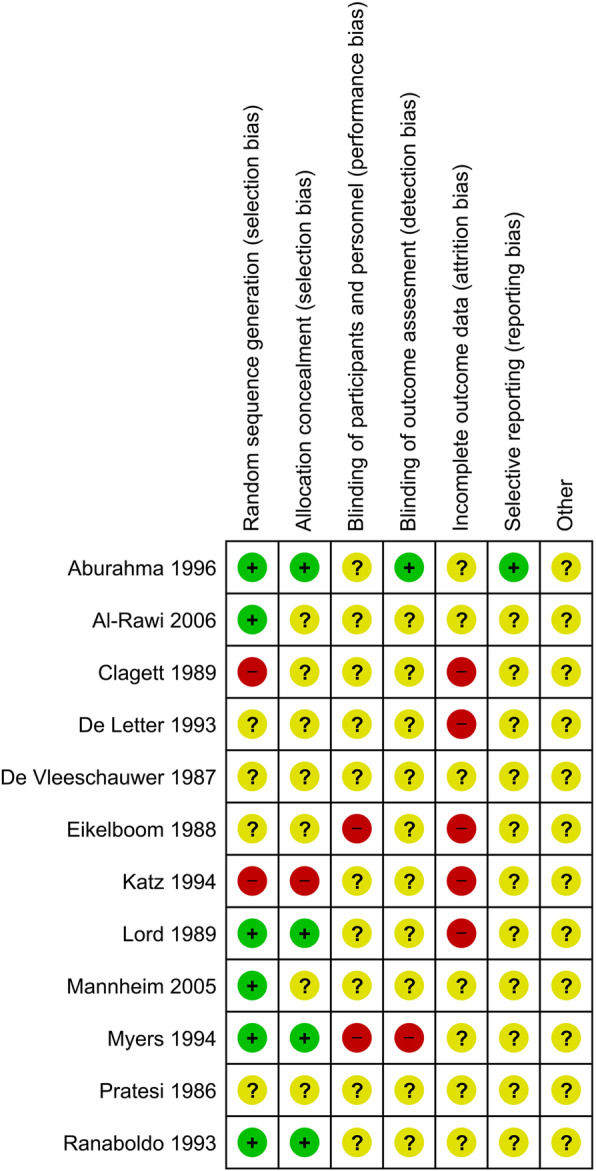
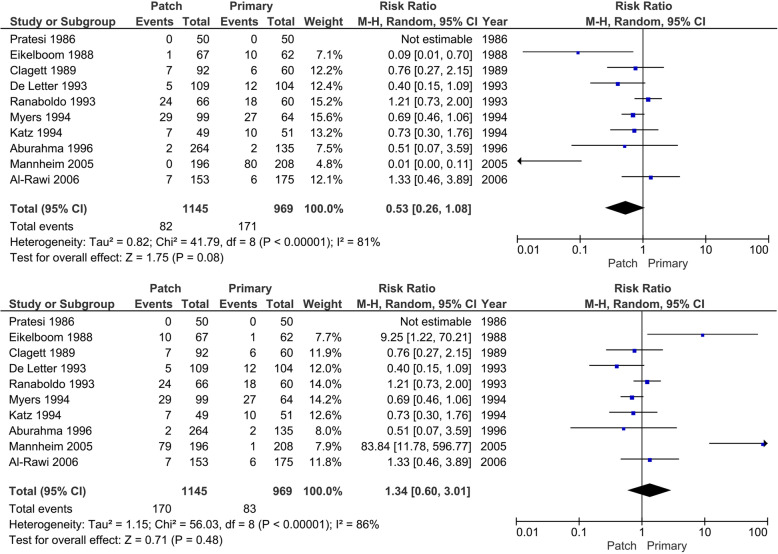
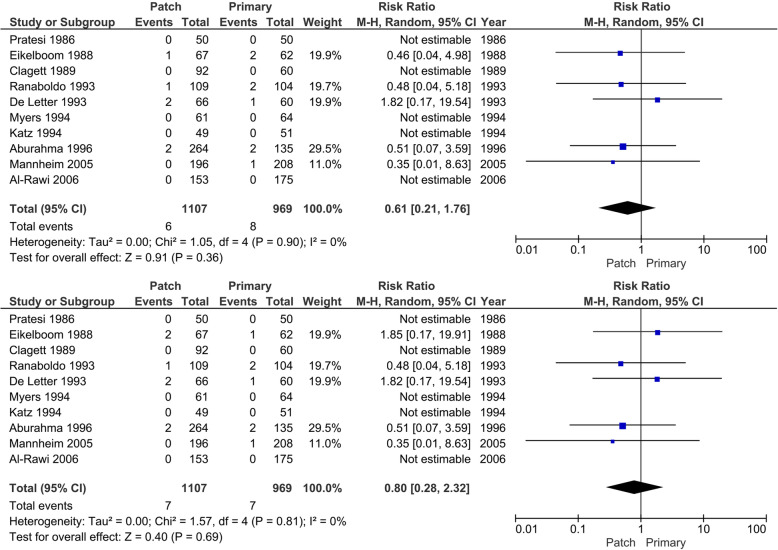
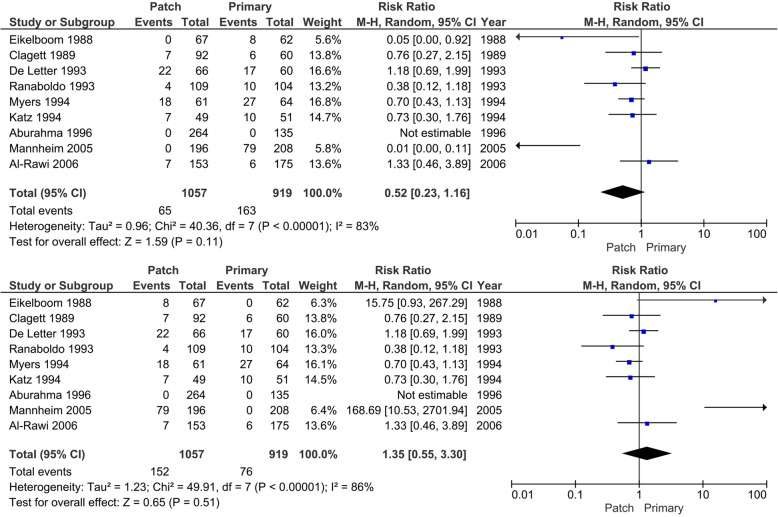
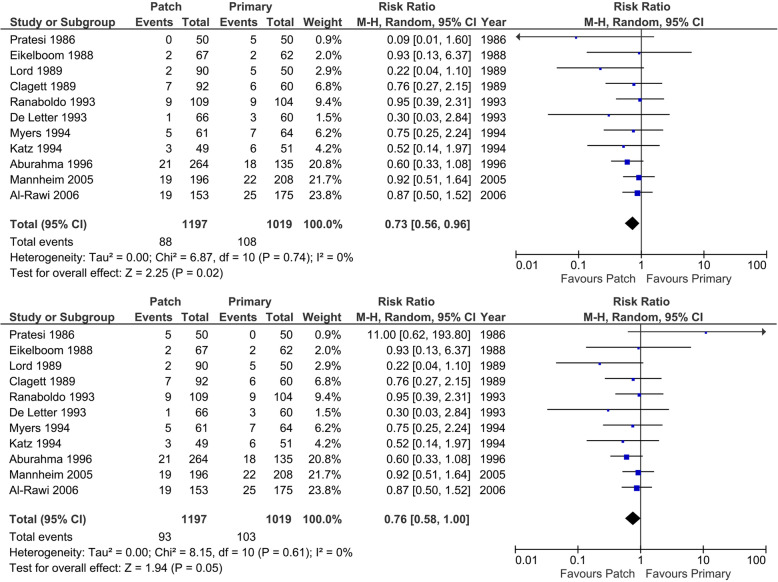
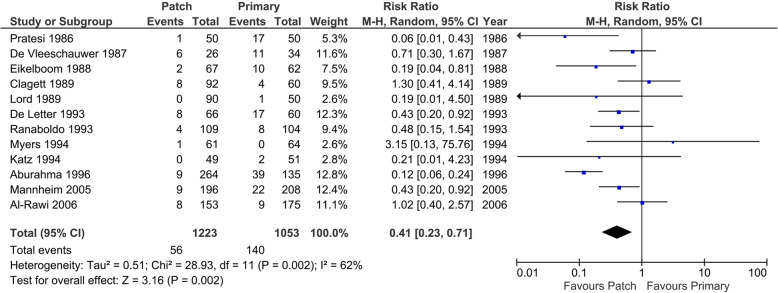
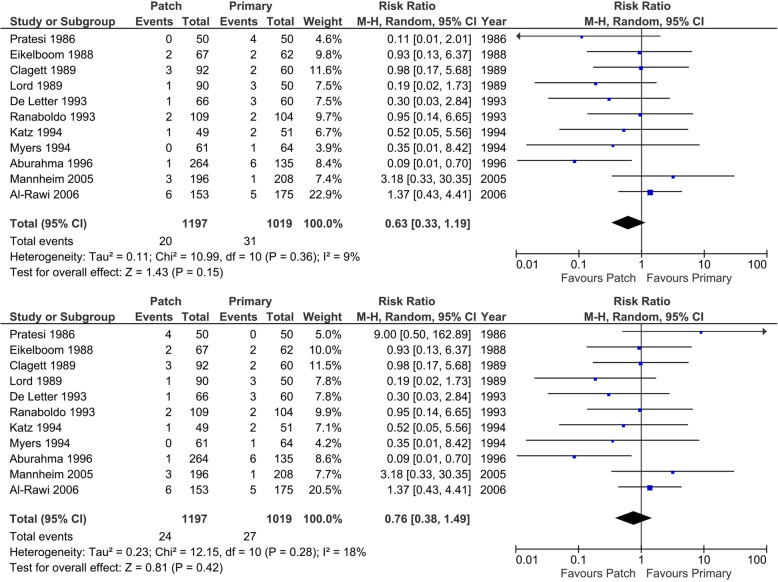
Results: We included 12 randomized clinical trials including 2187 participants who underwent 2335 operations for carotid stenosis comparing carotid endarterectomy with patch closure (1280 operations) versus carotid endarterectomy with primary closure (1055 operations). Meta-analysis comparing carotid endarterectomy with patch angioplasty versus carotid endarterectomy with primary closure may potentially decrease the number of patients with all-cause mortality (RR 0.53; 95% CI 0.26 to 1.08; p = 0.08, best-case scenario for patch), serious adverse events (RR 0.73; 95% CI 0.56 to 0.96; p = 0.02, best-case scenario for patch), and the number of restenosis (RR 0.41; 95% CI 0.23 to 0.71; p < 0.01). Trial sequential analysis demonstrated that the required information sizes were far from being reached for these patient-important outcomes. All the patient-relevant outcomes were at low certainty of evidence according to The Grading of Recommendations Assessment, Development, and Evaluation.
Conclusions: This systematic review showed no conclusive evidence of a difference between carotid endarterectomy with patch angioplasty versus primary closure of the arterial wall on all-cause mortality, < 30 days mortality, < 30 days stroke, or any other serious adverse events. These conclusions are based on data from 15 to 35 years ago, obtained in trials with very low certainty according to GRADE, and should be interpreted cautiously. Therefore, we suggest conducting new randomized clinical trials patch angioplasty versus primary closure in carotid endarterectomy in symptomatic patients with an internal carotid artery stenosis of 50% or more. Such trials ought to be designed according to the Standard Protocol Items: Recommendations for Interventional Trials statement (Chan et al., Ann Intern Med 1:200-7, 2013) and reported according to the Consolidated Standards of Reporting Trials statement (Schulz et al., 7, 2010). Until conclusive evidence is obtained, the standard of care according to guidelines should not be abandoned.
Systematic review registration: PROSPERO CRD42014013416 . Review protocol publication 2019 DOI: https://doi.org/10.1136/bmjopen-2018-026419 .
Keywords: Carotid endarterectomy; Carotid stenosis; GRADE; Patch; Primary closure; Systematic review; Trial sequential analysis.
Conflict of interest statement
We have no known conflicts of interest to disclose apart from the following. Jørn Wetterslev and Christian Gluud are members of the taskforce at Copenhagen Trial Unit (CTU) to develop theory and software for doing trial sequential analysis (TSA) currently freeware available including a manual at
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
