

Cardiovascular disease risk prevention services by pharmacists in Saudi Arabia: what do policymakers and opinion leaders think?
- PMID: 33958004
- PMCID: PMC8100751
- DOI: 10.1186/s40545-021-00319-6
Cardiovascular disease risk prevention services by pharmacists in Saudi Arabia: what do policymakers and opinion leaders think?
Abstract
Background: Cardiovascular disease (CVD) is an emerging contributor to national morbidity and mortality in Saudi Arabia. CVD risk prevention services are limited, particularly with an over-utilised public health sector and an under-utilised and under-resourced primary care sector. Globally, there is evidence that community pharmacists can play a key role in CVD prevention within primary care. However, the perspectives of policymakers and opinion leaders are critical to successful translation of evidence into practice. Thus, the aim was to engage policymakers and professional leaders in discussions about implementing high-quality CVD risk prevention services in community pharmacy.
Methods: Qualitative semi-structured interviews were conducted, audio-recorded and transcribed verbatim. All transcripts were thematically analysed.
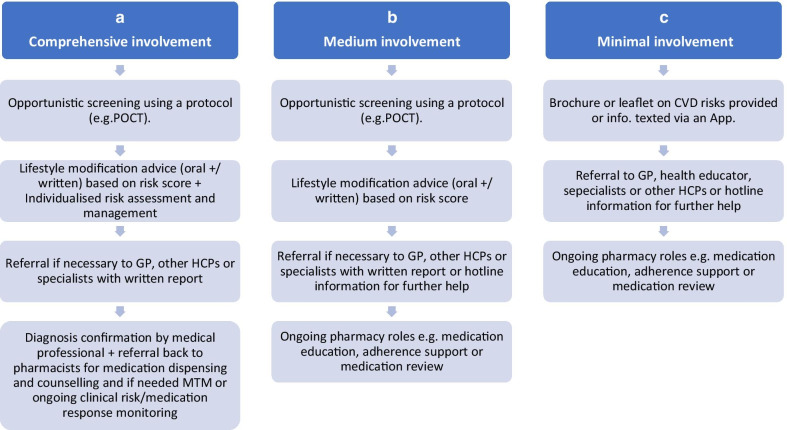
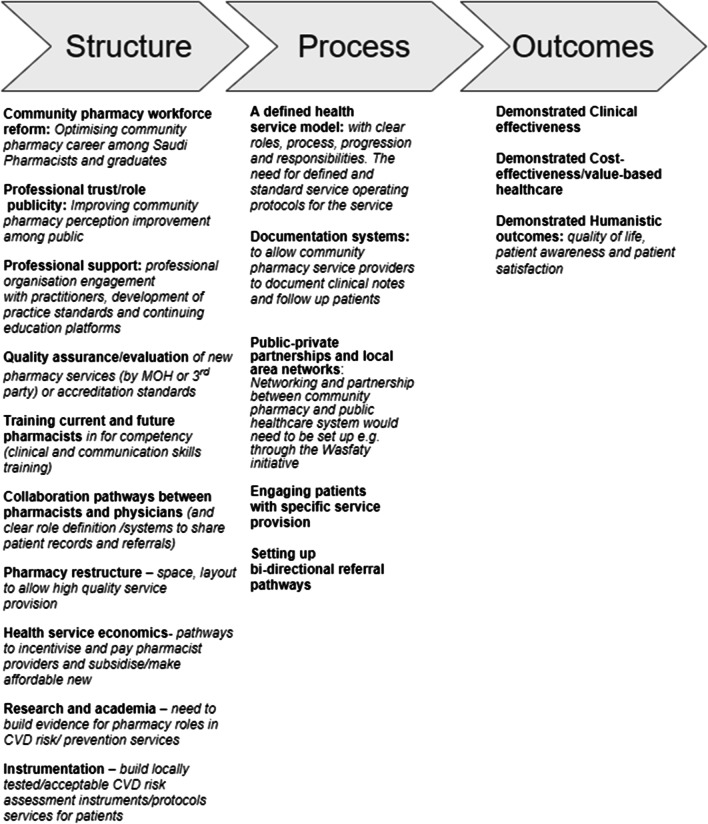
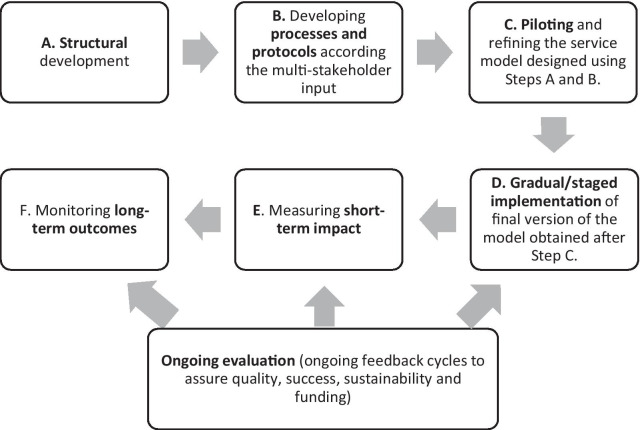
Results: A total of 23 participants (87% male) from government and non-government sectors were interviewed. Of these, almost 65% had pharmacy qualifications. Limited provision of CVD risks preventative services in primary care was acknowledged by most participants and building community pharmacists' capacity to assist in preventive health services was viewed favourably as one way of improving the status quo. The data yielded four key themes: (1) future pharmacy CVD health service models; (2) demonstrable outcomes; (3) professional engagement and advocacy; and (4) implementability. CVD health services roles (health screening, primary and secondary prevention services), pragmatic factors and tiered models of care (minimal, medium, and comprehensive pharmacist involvement) were discussed. The need for humanistic, clinical, and cost effectiveness outcomes to be demonstrated and active involvement of professional bodies were deemed important for such services to be sustainable. Professional pharmacy governance to develop pharmacy careers and workforce, pharmacy curricular reform and ongoing education were posed as key success factors for novel pharmacy roles. Practice policies, standards, and guidelines were seen as required to adhere to stringent quality control for future pharmacy services provision. Participant's implementation vision for such services included scalability, affordability, access, adoption and health system reform. Most discussions focused on the need for structural improvement with limited input regarding processes or outcomes required to establish such models.
Conclusions: Most participants favoured pharmacy-based CVD risk prevention services, despite the variability in proposed service models. However, prior to developing such services, support structures at the health system and health professional level are needed as well as building public support and acceptability for pharmacy services.
Keywords: CVD risk prevention services; Pharmacists; Pharmacy services; Policymakers; System reform.
Conflict of interest statement
The authors report no competing interest.
Figures
Similar articles
-
Cardiovascular disease risk screening by pharmacists: a behavior change wheel guided qualitative analysis.Res Social Adm Pharm. 2020 Feb;16(2):149-159. doi: 10.1016/j.sapharm.2019.04.009. Epub 2019 Apr 16. Res Social Adm Pharm. 2020. PMID: 31027964
-
Health consumer engagement in developing novel preventive health community pharmacy roles in cardiovascular disease in Saudi Arabia: A qualitative analysis.Saudi Pharm J. 2020 May;28(5):529-537. doi: 10.1016/j.jsps.2020.03.004. Epub 2020 Mar 18. Saudi Pharm J. 2020. PMID: 32435133 Free PMC article.
-
Physicians' views on cardiovascular disease risk prevention services by pharmacists and potential for collaboration.Explor Res Clin Soc Pharm. 2021 Sep 29;4:100077. doi: 10.1016/j.rcsop.2021.100077. eCollection 2021 Dec. Explor Res Clin Soc Pharm. 2021. PMID: 35479842 Free PMC article.
-
Multi-stakeholder perspective on community pharmacy services in Saudi Arabia: A systematic review and meta-analyses for 2010-2020.Explor Res Clin Soc Pharm. 2025 Apr 28;18:100608. doi: 10.1016/j.rcsop.2025.100608. eCollection 2025 Jun. Explor Res Clin Soc Pharm. 2025. PMID: 40417230 Free PMC article. Review.
-
Infectious diseases pharmacy practice, education, and research in Saudi Arabia: A review and future perspectives by the Infectious Diseases Pharmacy Specialty Network at the Saudi Society of Clinical Pharmacy.Saudi Pharm J. 2022 Dec;30(12):1836-1843. doi: 10.1016/j.jsps.2022.10.014. Epub 2022 Nov 3. Saudi Pharm J. 2022. PMID: 36601505 Free PMC article. Review.
Cited by
-
Prevalence, hematological parameters, and coagulation profiles: Cardiovascular diseases statistics in the Asir region, Saudi Arabia.Saudi Med J. 2023 Apr;44(4):385-393. doi: 10.15537/smj.2023.44.4.20220746. Saudi Med J. 2023. PMID: 37062554 Free PMC article.
-
Cardiovascular Disease-Related Health Promotion and Prevention Services by Pharmacists in Saudi Arabia: How Well Are They Prepared?Healthcare (Basel). 2023 May 31;11(11):1614. doi: 10.3390/healthcare11111614. Healthcare (Basel). 2023. PMID: 37297754 Free PMC article.
-
A stakeholders' perspective on enhancing community pharmacists' roles in controlling non-communicable diseases in the United Arab Emirates.J Pharm Policy Pract. 2024 Sep 20;17(1):2404080. doi: 10.1080/20523211.2024.2404080. eCollection 2024. J Pharm Policy Pract. 2024. PMID: 39314667 Free PMC article.
-
Patient journey for hypertension and dyslipidemia in Saudi Arabia: highlighting the evidence gaps.Arch Public Health. 2023 Jul 3;81(1):122. doi: 10.1186/s13690-023-01121-3. Arch Public Health. 2023. PMID: 37400868 Free PMC article.
-
Stakeholders' perceptions and experiences of factors influencing the commissioning, delivery, and uptake of general health checks: a qualitative evidence synthesis.Cochrane Database Syst Rev. 2025 Mar 20;3(3):CD014796. doi: 10.1002/14651858.CD014796.pub2. Cochrane Database Syst Rev. 2025. PMID: 40110911
References
-
- Buss VH, Shield A, Kosari S, Naunton M. The impact of clinical services provided by community pharmacies on the Australian healthcare system: a review of the literature. J Pharm Policy Pract. 2018;11(1):22. doi: 10.1186/s40545-018-0149-7. - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources