

Patient delay and benefit of timely reperfusion in ST-segment elevation myocardial infarction
- PMID: 33958491
- PMCID: PMC8103948
- DOI: 10.1136/openhrt-2021-001650
Patient delay and benefit of timely reperfusion in ST-segment elevation myocardial infarction
Abstract
Background: In patients with ST-segment elevation myocardial infarction (STEMI), it is unknown how patient delay modulates the beneficial effects of timely reperfusion.
Aims: To assess the prognostic significance of a contact-to-balloon time of less than 90 min on in-hospital mortality in different categories of symptom-onset-to-first-medical-contact (S2C) times.
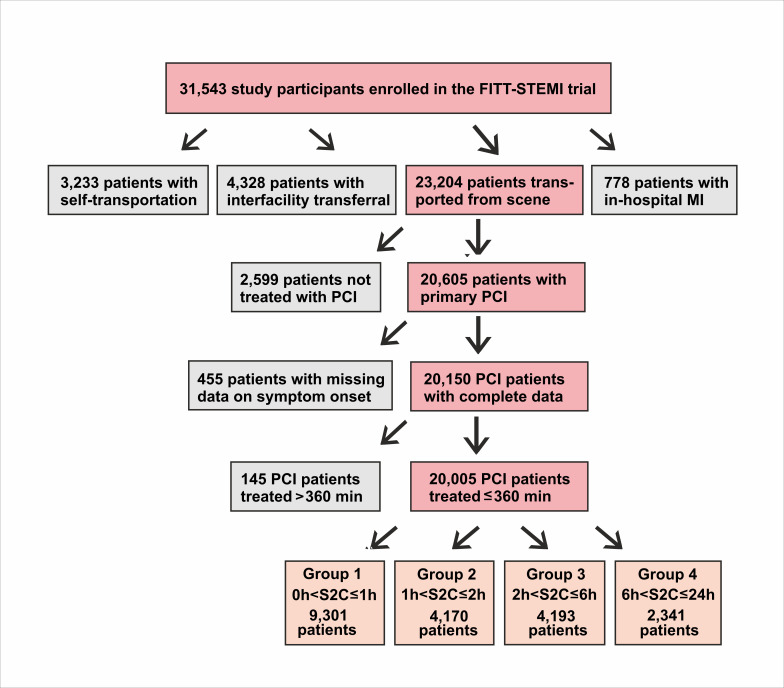
Methods: A total of 20 005 consecutive patients from the Feedback Intervention and Treatment Times in ST-segment Elevation Myocardial Infarction (FITT-STEMI) programme treated with primary percutaneous coronary intervention (PCI) were included.
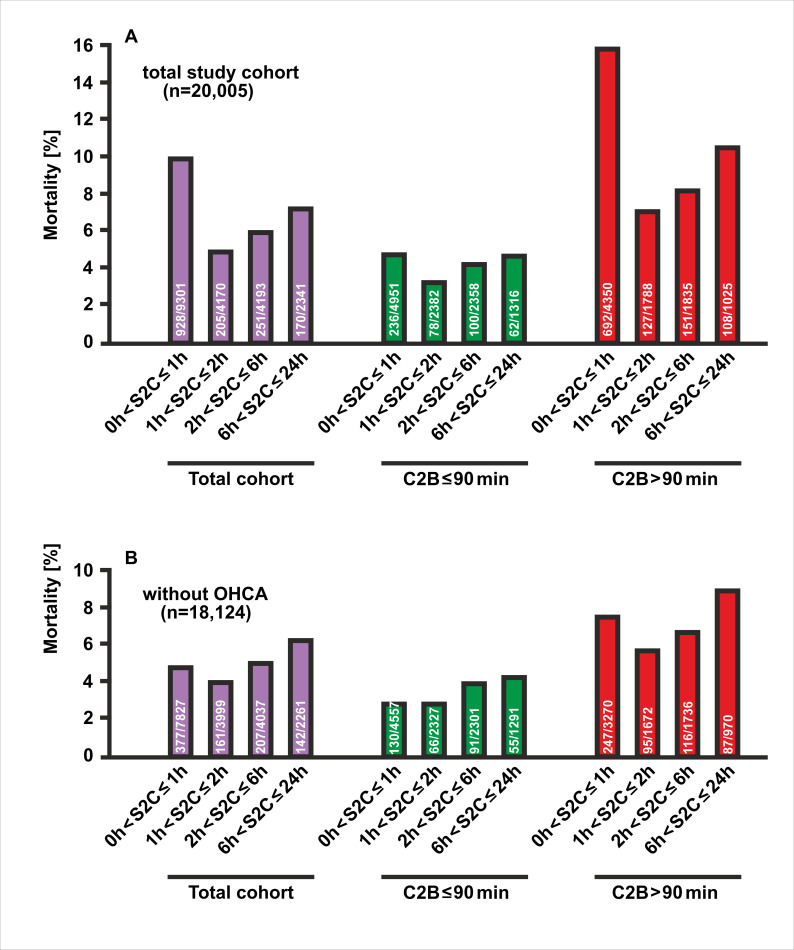
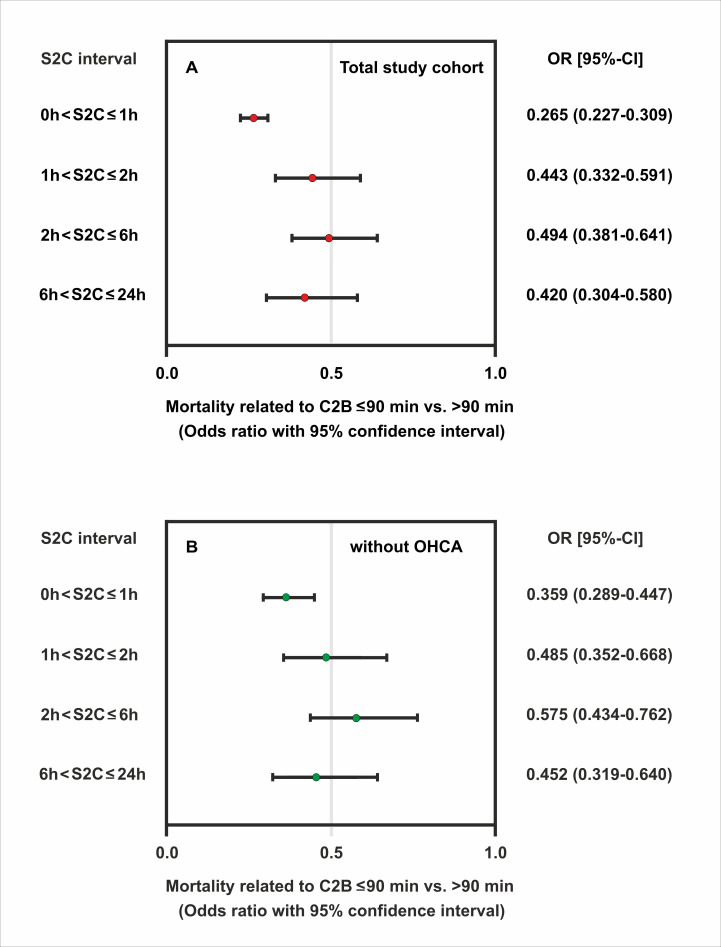
Results: There were 1554 deaths (7.8%) with a J-shaped relationship between mortality and S2C time. Mortality was 10.0% in patients presenting within 1 hour, and 4.9%, 6.0% and 7.3% in patient groups with longer S2C intervals of 1-2 hours, 2-6 hours and 6-24 hours, respectively. Patients with a short S2C interval of less than 1 hour (S2C<60 min) had the highest survival benefit from timely reperfusion with PCI within 90 min (OR 0.27, 95% CI 0.23 to 0.31, p<0.0001) as compared with the three groups with longer S2C intervals of 1 hour<S2C≤2 hours (OR 0.44, 95% CI 0.33 to 0.59, p<0.0001), 2 hours<S2C≤6 hours (OR 0.49, 95% CI 0.38 to 0.64, p<0.0001) and 6 hours<S2C≤24 hours (OR 0.42, 95% CI 0.30 to 0.58, p<0.0001).
Conclusions: Timely reperfusion with a contact-to-balloon time of less than 90 min is most effective in patients presenting with short S2C intervals of less than 1 hour, but has also beneficial effects in patients with S2C intervals of up to 24 hours.
Trial registration number: NCT00794001.
Keywords: acute coronary syndrome; chest pain; myocardial infarction.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: TF reports personal fees for consultancies (including data monitoring committees) from Novartis, Bayer, Biogen, AstraZeneca, Janssen, Grünenthal, Pharmalog, SGS, Boehringer Ingelheim, Daiichi-Sankyo, Mediconomics and Roche, all outside the submitted work. Furthermore, he has received research funding by the European Commission for statistical analyses on the EUTrigTreat (NCT01209494) and EU-CERT-ICD (NCT02064192) clinical studies. All relationships declared are modest.
Figures
References
-
- O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: Executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task force on Practice Quidelines. Circulation 2013;127:e529–55. 10.1161/CIR.0b013e3182742c84 - DOI - PubMed
-
- Ibanez B, James S, Agewall S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 2018;39:119–77. 10.1093/eurheartj/ehx393 - DOI - PubMed
-
- Scholz KH, Maier SKG, Maier LS, et al. Impact of treatment delay on mortality in ST-segment elevation myocardial infarction (STEMI) patients presenting with and without haemodynamic instability: results from the German prospective, multicentre FITT-STEMI trial. Eur Heart J 2018;39:1065–74. 10.1093/eurheartj/ehy004 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous