

A putative "chemokine switch" that regulates systemic acute inflammation in humans
- PMID: 33958628
- PMCID: PMC8102583
- DOI: 10.1038/s41598-021-88936-8
A putative "chemokine switch" that regulates systemic acute inflammation in humans
Abstract
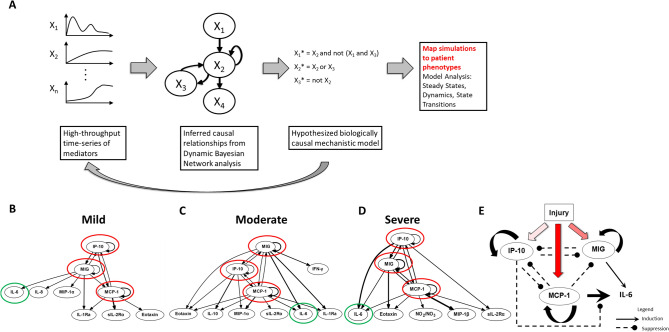
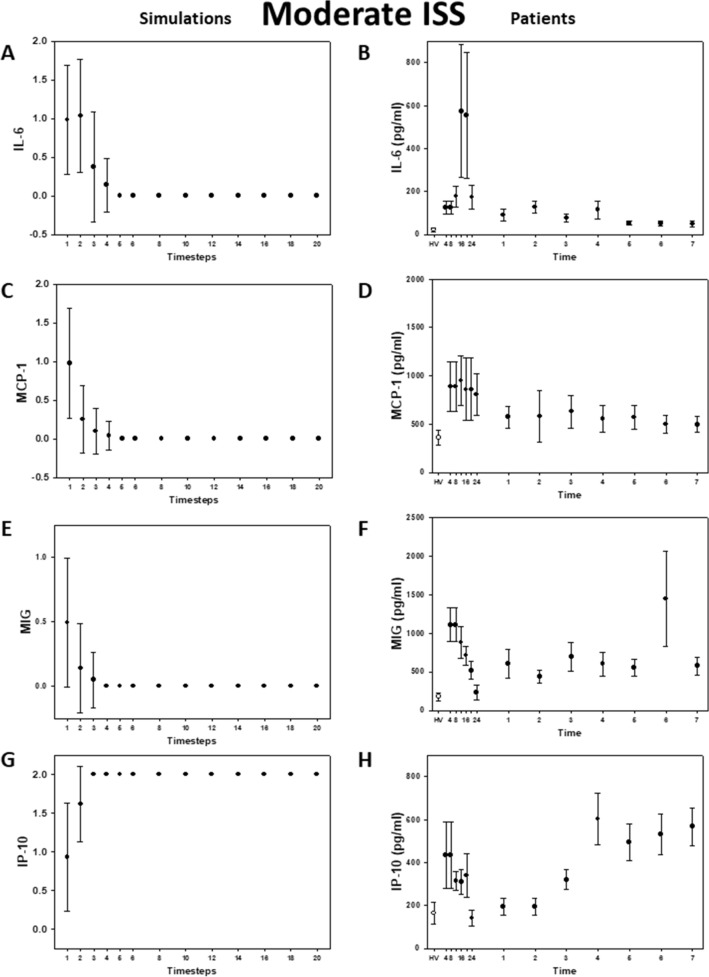
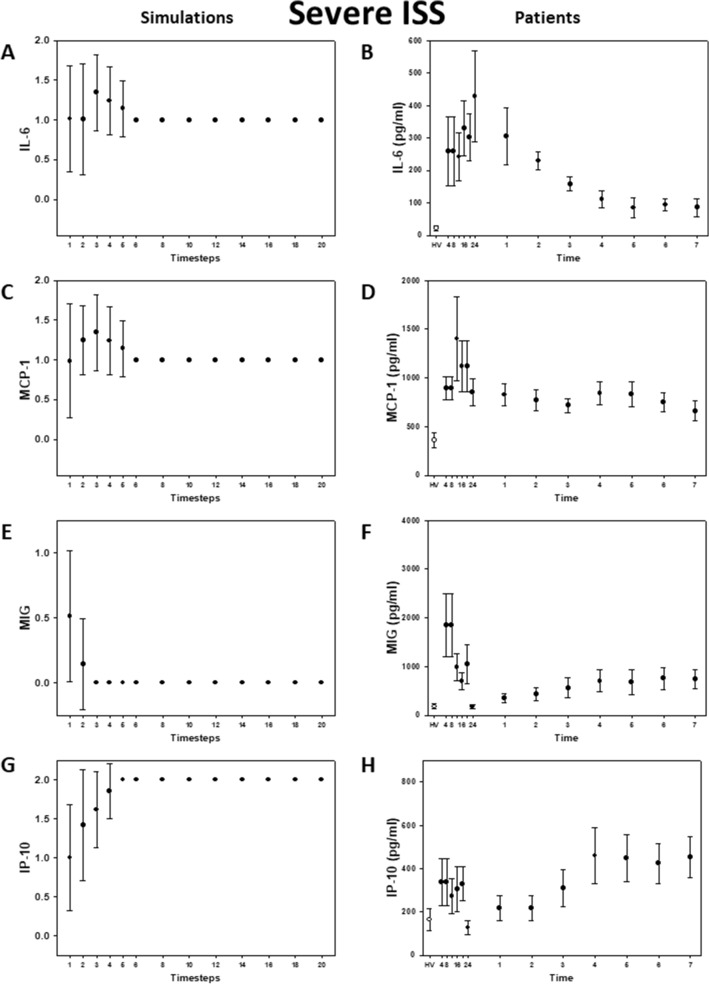
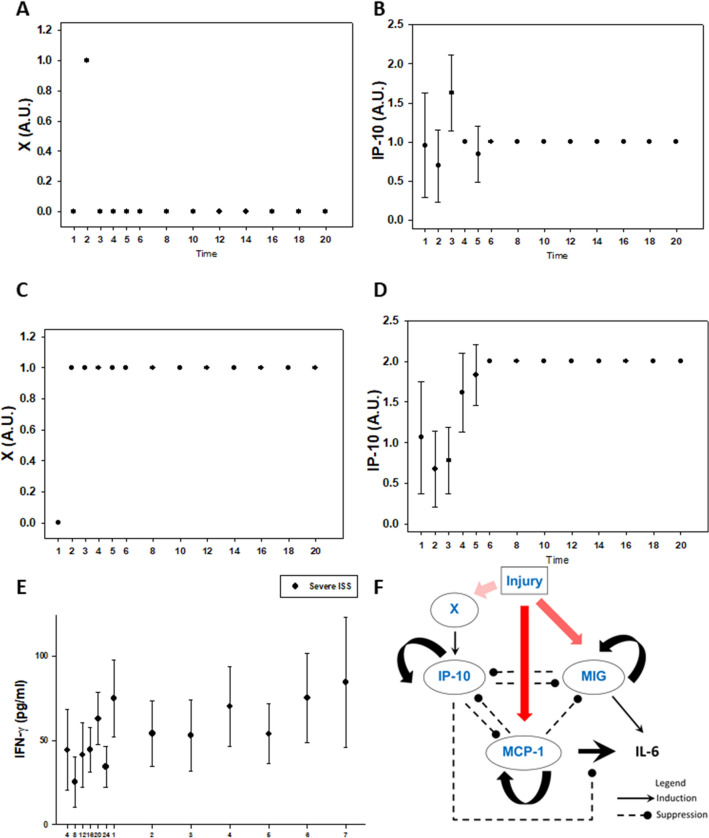
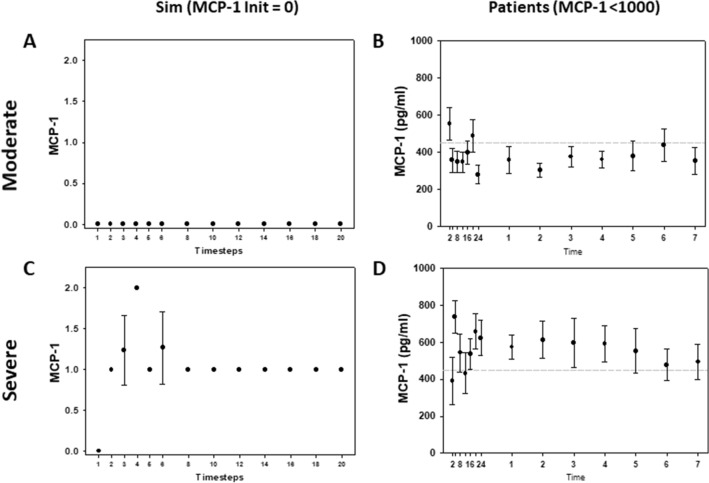
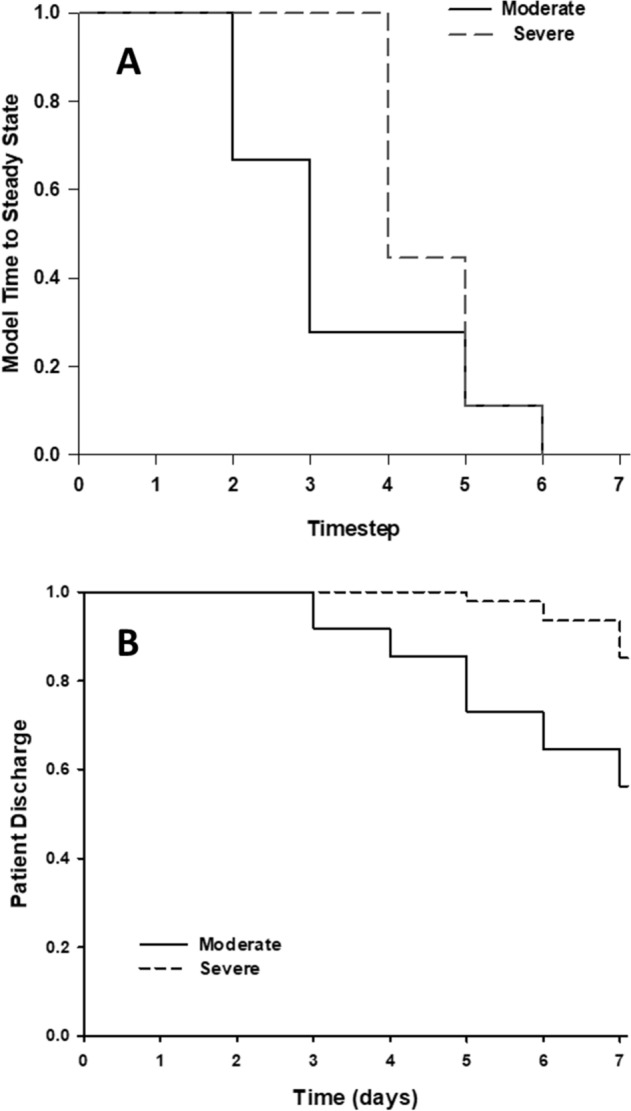
Systemic inflammation is complex and likely drives clinical outcomes in critical illness such as that which ensues following severe injury. We obtained time course data on multiple inflammatory mediators in the blood of blunt trauma patients. Using dynamic network analyses, we inferred a novel control architecture for systemic inflammation: a three-way switch comprising the chemokines MCP-1/CCL2, MIG/CXCL9, and IP-10/CXCL10. To test this hypothesis, we created a logical model comprising this putative architecture. This model predicted key qualitative features of systemic inflammation in patient sub-groups, as well as the different patterns of hospital discharge of moderately vs. severely injured patients. Thus, a rational transition from data to data-driven models to mechanistic models suggests a novel, chemokine-based mechanism for control of acute inflammation in humans and points to the potential utility of this workflow in defining novel features in other complex diseases.
Conflict of interest statement
NA, RN, KA, AZ, OAM, DB, JY, FE, AA, RLS, RZ and TRB have no competing interests. YV is a co-founder of, and stakeholder in, Immunetrics, Inc.
Figures
References
-
- Catania RA, Chaudry IH. Immunological consequences of trauma and shock. Ann. Acad Med. Singap. 1999;28:120–132. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
