

Radiomics and radiogenomics in gliomas: a contemporary update
- PMID: 33958734
- PMCID: PMC8405677
- DOI: 10.1038/s41416-021-01387-w
Radiomics and radiogenomics in gliomas: a contemporary update
Abstract
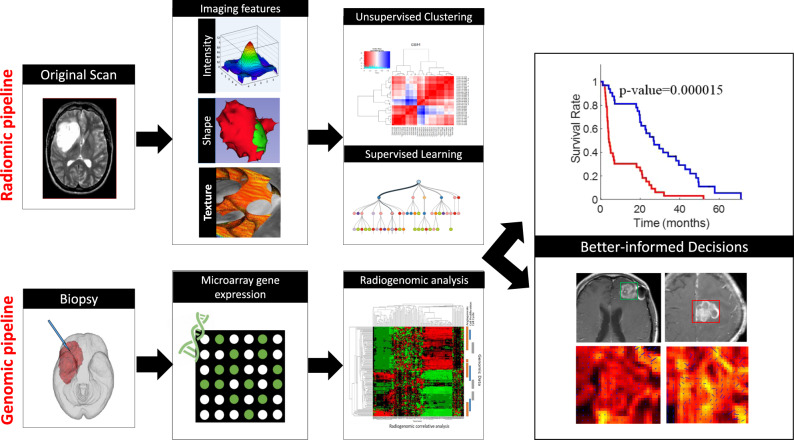
The natural history and treatment landscape of primary brain tumours are complicated by the varied tumour behaviour of primary or secondary gliomas (high-grade transformation of low-grade lesions), as well as the dilemmas with identification of radiation necrosis, tumour progression, and pseudoprogression on MRI. Radiomics and radiogenomics promise to offer precise diagnosis, predict prognosis, and assess tumour response to modern chemotherapy/immunotherapy and radiation therapy. This is achieved by a triumvirate of morphological, textural, and functional signatures, derived from a high-throughput extraction of quantitative voxel-level MR image metrics. However, the lack of standardisation of acquisition parameters and inconsistent methodology between working groups have made validations unreliable, hence multi-centre studies involving heterogenous study populations are warranted. We elucidate novel radiomic and radiogenomic workflow concepts and state-of-the-art descriptors in sub-visual MR image processing, with relevant literature on applications of such machine learning techniques in glioma management.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
