

Association of right ventricular dysfunction and pulmonary hypertension with adverse 30-day outcomes in COVID-19 patients
- PMID: 33959257
- PMCID: PMC8060770
- DOI: 10.1177/20458940211007040
Association of right ventricular dysfunction and pulmonary hypertension with adverse 30-day outcomes in COVID-19 patients
Abstract
Background: Cardiac manifestations in COVID-19 are multifactorial and are associated with increased mortality. The clinical utility and prognostic value of echocardiography in COVID-19 inpatients is not clearly defined. We aim to identify echocardiographic parameters that are associated with 30-day clinical outcomes secondary to COVID-19 hospitalization.
Methods: This retrospective cohort study was conducted in a large tertiary hospital in New York City during the COVID-19 pandemic. It included 214 adult inpatients with a laboratory-confirmed diagnosis of COVID-19 by reverse transcriptase polymerase chain reaction assay (RT-PCR) for SARS-CoV-2 on nasopharyngeal swab and had a transthoracic echocardiogram performed during the index hospitalization. Primary outcome was 30-day all-cause inpatient mortality. Secondary outcomes were 30-day utilization of mechanical ventilator support, vasopressors, or renal replacement therapy.
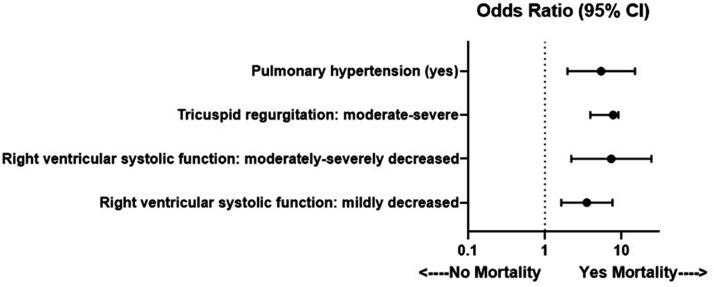
Results: Mild right ventricular systolic dysfunction (odds ratio (OR): 3.51, 95% confidence interval (CI): 1.63-7.57, p = 0.001), moderate to severe right ventricular systolic dysfunction (OR: 7.30, 95% CI: 2.20-24.25, p = 0.001), pulmonary hypertension (OR: 5.39, 95% CI: 1.96-14.86, p = 0.001), and moderate to severe tricuspid regurgitation (OR: 3.92, 95% CI: 1.71-9.03, p = 0.001) were each associated with increased odds of 30-day all-cause inpatient mortality. Pulmonary hypertension and moderate to severe right ventricular dysfunction were each associated with increased odds of 30-day utilization of mechanical ventilator support and vasopressors.
Conclusions: Right ventricular dysfunction, pulmonary hypertension, and moderate to severe tricuspid regurgitation were associated with increased odds for 30-day inpatient mortality. This study highlights the importance of echocardiography and its clinical utility and prognostic value for evaluating hospitalized COVID-19 patients.
Keywords: COVID-19; echocardiography; pulmonary hypertension; right ventricular dysfunction.
© The Author(s) 2021.
Conflict of interest statement
Conflict of interest: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K. W. P. served on an advisory board for Actelion and receives grant funding from United Therapeutics.
Figures
References
-
- COVID-19 Data, www1.nyc.gov/site/doh/covid/covid-19-data.page (accessed 7 September 2020).
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
