

Association Between the Pretreatment Albumin-to-Alkaline Phosphatase Ratio and Clinical Outcomes in Patients With Bladder Cancer Treated With Radical Cystectomy: A Retrospective Cohort Study
- PMID: 33959511
- PMCID: PMC8093628
- DOI: 10.3389/fonc.2021.664392
Association Between the Pretreatment Albumin-to-Alkaline Phosphatase Ratio and Clinical Outcomes in Patients With Bladder Cancer Treated With Radical Cystectomy: A Retrospective Cohort Study
Abstract
Objective: Serum albumin-to-alkaline phosphatase ratio (AAPR) has been proven to be a prognostic indicator of many malignant tumors. However, whether it can predict the prognosis of bladder cancer (BC) patients who underwent radical cystectomy (RC) remains unclear. This study was designed to assess the relationship between AAPR and clinical outcomes in patients with BC treated with RC.
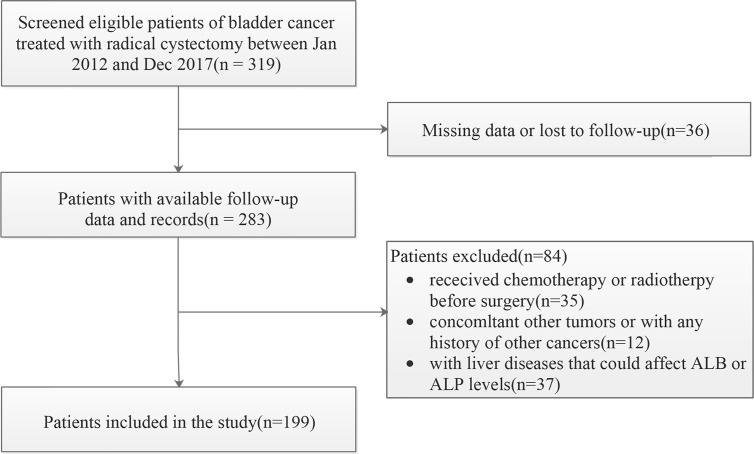
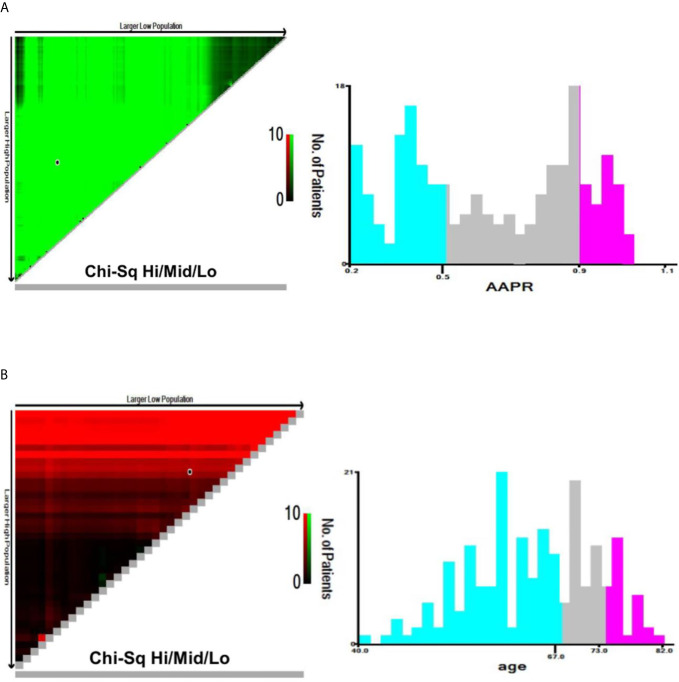
Methods: The clinicopathological data of 199 BC patients receiving RC in our institution from January 2012 to December 2017 were retrospectively collected and analyzed. They were divided into three groups based on the optimal cut-off values and the association between AAPR groups and their clinical outcomes were evaluated.
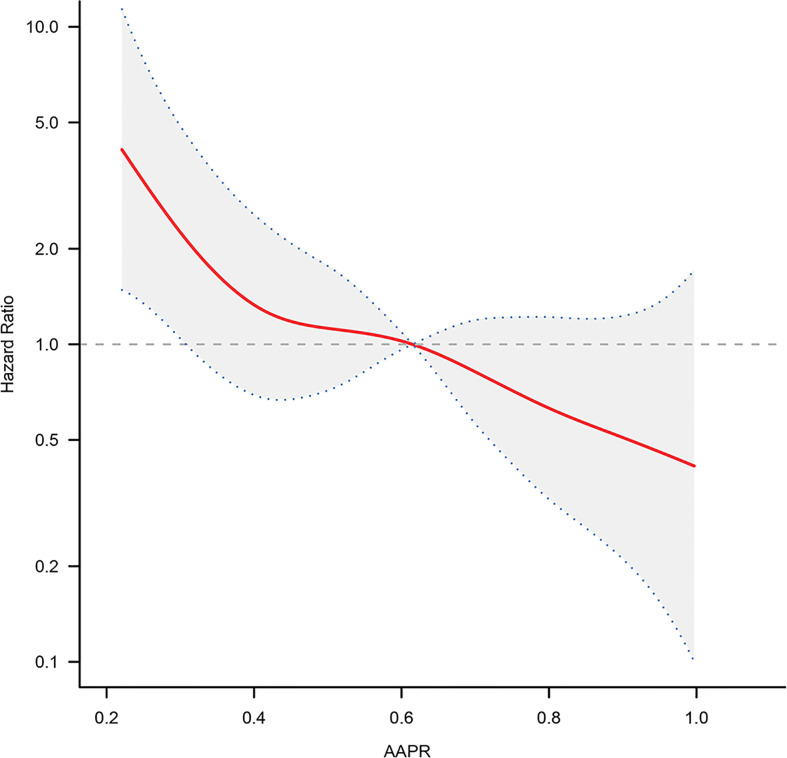
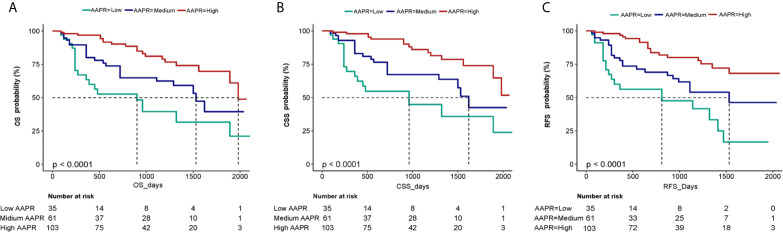
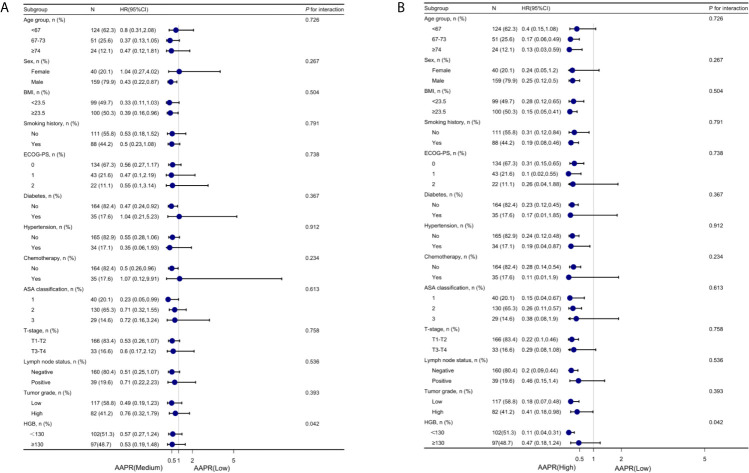
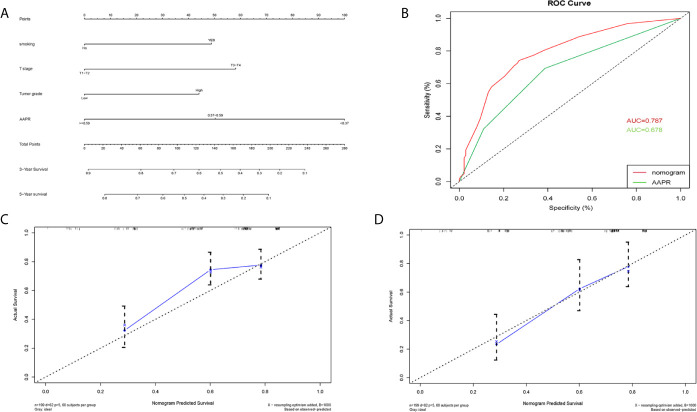
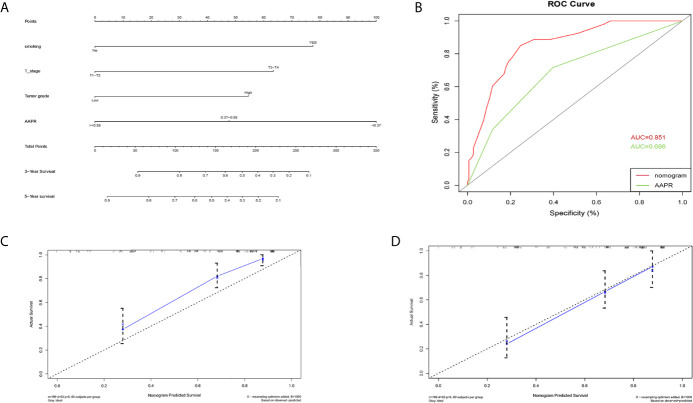
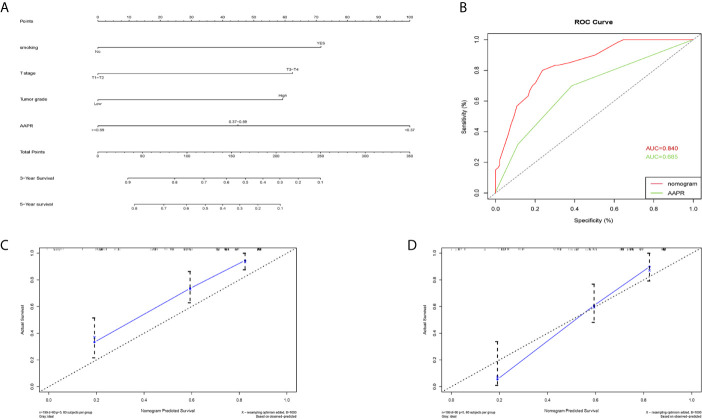
Results: The average age of the patients was (64.0 ± 8.7) years and 79.9% were male. Based on the cut-off values of AAPR, patients were divided into three groups: low-AAPR group (AAPR < 0.37, n = 35), medium-AAPR group (AAPR = 0.37-0.59, n = 61) and high-AAPR group (AAPR > 0.59, n = 103). The median overall survival (OS) of each AAPR group was 12.5, 24, and 29 months, respectively (P value <0.0001). After adjusting the Cox proportional hazards model, medium- and high- AAPR groups showed a reduced risk trend of death, with a risk ratio of 0.44 (95% CI = 0.21-0.91) and 0.25 (95% CI = 0.12-0.49), respectively (P for trend <0.001). No nonlinear relationship was identified by smooth fitting curve between AAPR and OS. By subgroup analysis, we observed that compared to the low-AAPR group, the trends of the HRs in the medium- and high-AAPR group were decreased across nearly all subgroups after stratification. Moreover, the AAPR-based nomograms for OS, CSS and RFS were also constructed. The C-index showed a good predictive accuracy (OS, C-index 0.728, 95% CI 0.663-0.793; CSS, C-index 0.792, 95% CI 0.748-0.838; RFS, C-index 0.784, 95% CI 0.739-0.829).
Conclusion: Pretreatment AAPR is significantly associated with the prognosis of BC patients receiving RC, which can be conducive to the clinical decision-making and risk stratification in those patients. The nomogram based on AAPR is a reliable model for predicting survival of BC patients after RC.
Keywords: albumin-to-alkaline phosphatase ratio; bladder cancer; nomogram; prognostic impact; radical cystectomy.
Copyright © 2021 Li, Lu, Liu and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Prognostic value of preoperative albumin-to-alkaline phosphatase ratio in patients with surgically treated urological cancer: a systematic review and meta-analysis.Front Oncol. 2023 Nov 9;13:1236167. doi: 10.3389/fonc.2023.1236167. eCollection 2023. Front Oncol. 2023. PMID: 38023164 Free PMC article.
-
Prognostic Value of Preoperative Albumin-to-Alkaline Phosphatase Ratio in Patients with Muscle-Invasive Bladder Cancer After Radical Cystectomy.Onco Targets Ther. 2020 Dec 29;13:13265-13274. doi: 10.2147/OTT.S285098. eCollection 2020. Onco Targets Ther. 2020. PMID: 33402835 Free PMC article.
-
The Prognostic Value of Preoperative Albumin-to-Alkaline Phosphatase Ratio on Survival Outcome for Patients With Locally Advanced Oral Squamous Cell Carcinoma.Technol Cancer Res Treat. 2022 Jan-Dec;21:15330338221141254. doi: 10.1177/15330338221141254. Technol Cancer Res Treat. 2022. PMID: 36426570 Free PMC article.
-
Predictive value of pretreatment albumin-to-alkaline phosphatase ratio for overall survival for patients with advanced non-small cell lung cancer.Cancer Med. 2020 Sep;9(17):6268-6280. doi: 10.1002/cam4.3244. Epub 2020 Jul 21. Cancer Med. 2020. PMID: 32691996 Free PMC article.
-
Prognostic effect of albumin-to-alkaline phosphatase ratio on patients with hepatocellular carcinoma: a systematic review and meta-analysis.Sci Rep. 2023 Jan 31;13(1):1808. doi: 10.1038/s41598-023-28889-2. Sci Rep. 2023. PMID: 36720974 Free PMC article.
Cited by
-
Development and validation of a nomogram prediction model based on albumin-to-alkaline phosphatase ratio for predicting the prognosis of gallbladder carcinoma.Pathol Oncol Res. 2023 Jan 4;28:1610818. doi: 10.3389/pore.2022.1610818. eCollection 2022. Pathol Oncol Res. 2023. PMID: 36685104 Free PMC article.
-
Prognostic value of preoperative albumin-to-alkaline phosphatase ratio in patients with surgically treated urological cancer: a systematic review and meta-analysis.Front Oncol. 2023 Nov 9;13:1236167. doi: 10.3389/fonc.2023.1236167. eCollection 2023. Front Oncol. 2023. PMID: 38023164 Free PMC article.
-
Comparative efficacy of Bacillus Calmette-Guérin instillation and radical cystectomy treatments for high-risk non-muscle-invasive urothelial cancer classified as high-grade T1 in initial and repeat transurethral resection of bladder tumor.Front Oncol. 2024 Jun 18;14:1394451. doi: 10.3389/fonc.2024.1394451. eCollection 2024. Front Oncol. 2024. PMID: 38957323 Free PMC article.
-
Predicting 3-year all-cause mortality in rectal cancer patients based on body composition and machine learning.Front Nutr. 2025 Mar 3;12:1473952. doi: 10.3389/fnut.2025.1473952. eCollection 2025. Front Nutr. 2025. PMID: 40098743 Free PMC article.
-
Prognostic role of pre-treatment serum ALB in Patients with oropharyngeal cancer: A retrospective cohort study.Front Oncol. 2022 Oct 13;12:924210. doi: 10.3389/fonc.2022.924210. eCollection 2022. Front Oncol. 2022. PMID: 36531036 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources