

Entodermoscopy Update: A Contemporary Review on Dermoscopy of Cutaneous Infections and Infestations
- PMID: 33959518
- PMCID: PMC8088165
- DOI: 10.4103/idoj.IDOJ_559_20
Entodermoscopy Update: A Contemporary Review on Dermoscopy of Cutaneous Infections and Infestations
Abstract
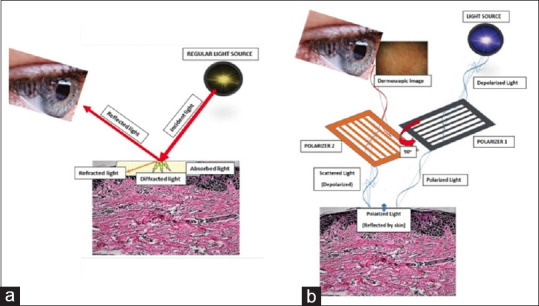
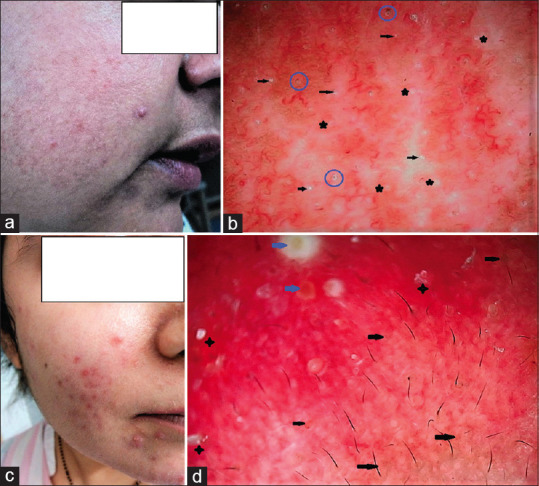
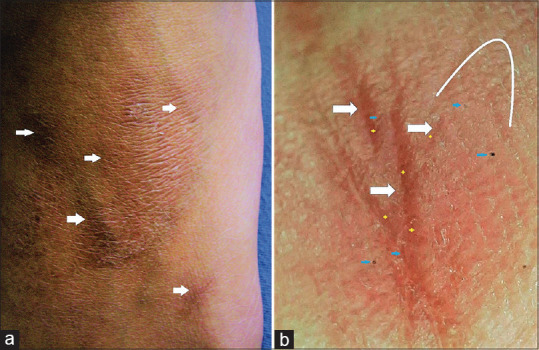
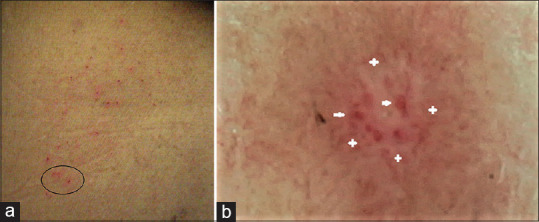
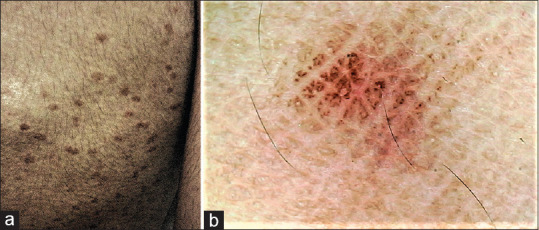
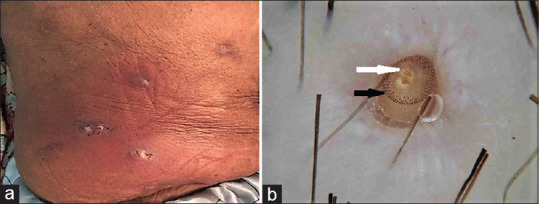
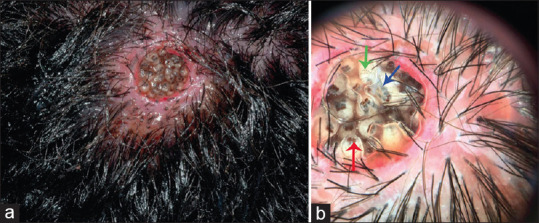
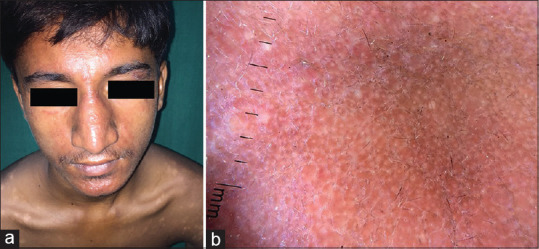
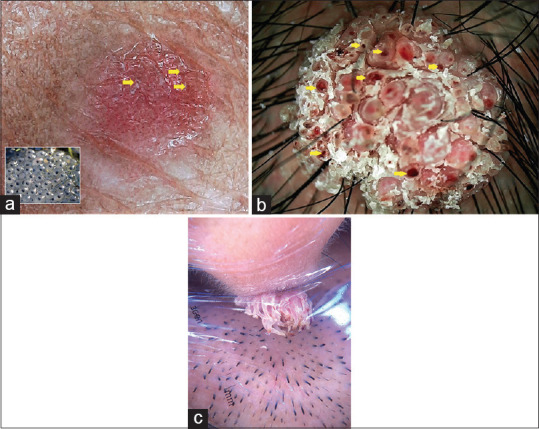
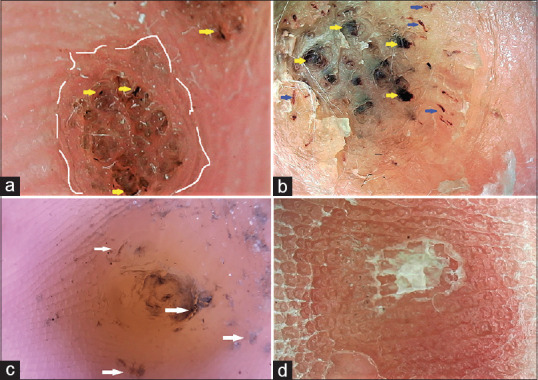
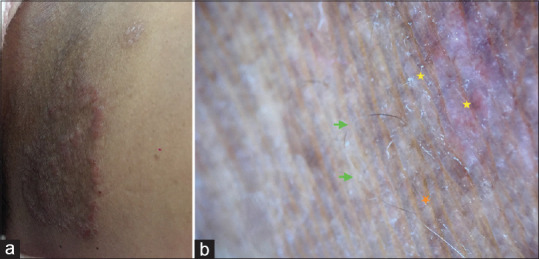
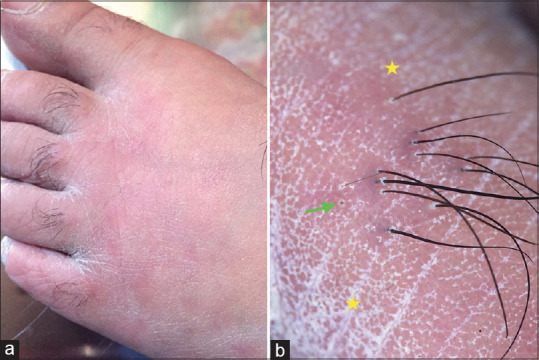
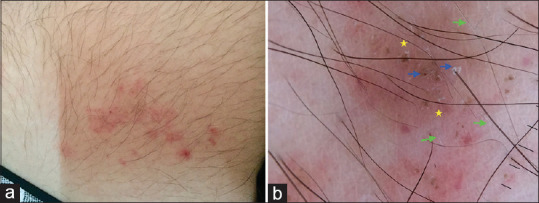
Infectious cutaneous diseases are very common, especially in certain geographic and tropical regions. Sometimes they may simulate other dermatoses, ordering verification of diagnosis with particular investigations. Dermoscopy is among one of the most important tools readily available in the outpatient setting for the dermatologist to confirm the diagnosis. In this up-to date review, literature concerning the various dermoscopic features of parasitic, viral, dermatophytic and bacterial cutaneous infections is composed. In addition artefacts as well as practical issues in dermoscopy usage are discussed; with the aim to empower dermatologists to promptly and non-invasively diagnose and manage cutaneous infections and infestations.
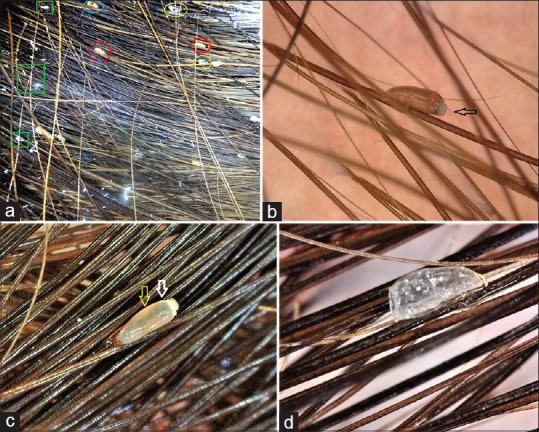
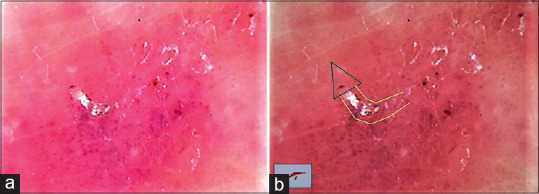
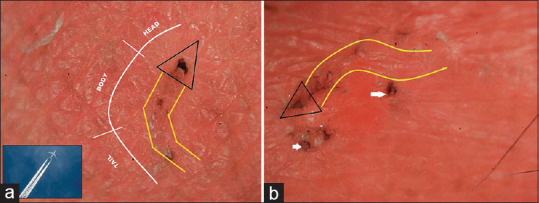
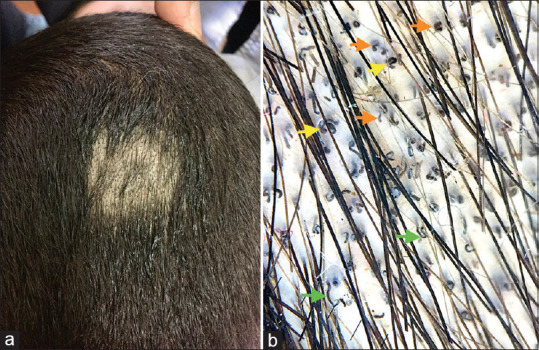
Keywords: Cutaneous infections; demodex; dermatophyte; dermatoscopy; dermoscopy; entodermoscopy; infestations; mite; molluscum; pediculosis; scabies; tinea; warts.
Copyright: © 2021 Indian Dermatology Online Journal.
Conflict of interest statement
There are no conflicts of interest.
Figures



Similar articles
-
Significance of dermatoscopy in genital dermatoses.Clin Dermatol. 2014 Mar-Apr;32(2):315-8. doi: 10.1016/j.clindermatol.2013.08.016. Clin Dermatol. 2014. PMID: 24559569 Review.
-
Dermoscopy of skin infestations and infections (entomodermoscopy) - Part II: viral, fungal and other infections.An Bras Dermatol. 2021 Nov-Dec;96(6):746-758. doi: 10.1016/j.abd.2021.04.008. Epub 2021 Oct 5. An Bras Dermatol. 2021. PMID: 34620527 Free PMC article. Review.
-
Exploring Pediatric Dermatology in Skin of Color: Focus on Dermoscopy.Life (Basel). 2024 Dec 4;14(12):1604. doi: 10.3390/life14121604. Life (Basel). 2024. PMID: 39768312 Free PMC article. Review.
-
Dermoscopy of skin infestations and infections (entomodermoscopy) - Part I: dermatozoonoses and bacterial infections.An Bras Dermatol. 2021 Nov-Dec;96(6):735-745. doi: 10.1016/j.abd.2021.04.007. Epub 2021 Oct 5. An Bras Dermatol. 2021. PMID: 34620524 Free PMC article. Review.
-
The Mite-Gallery Unit: A New Concept for Describing Scabies through Entodermoscopy.Trop Med Infect Dis. 2019 Mar 16;4(1):48. doi: 10.3390/tropicalmed4010048. Trop Med Infect Dis. 2019. PMID: 30884795 Free PMC article.
Cited by
-
Videodermoscopy in the Assessment of Patients With Ocular Demodicosis.Dermatol Pract Concept. 2023 Apr 1;13(2):e2023109. doi: 10.5826/dpc.1302a109. Online ahead of print. Dermatol Pract Concept. 2023. PMID: 37196309 Free PMC article.
-
Phthiriasis Palpebrarum: Dermoscopy to Rescue.Indian Dermatol Online J. 2025 Jan 20;16(2):352-353. doi: 10.4103/idoj.idoj_617_24. eCollection 2025 Mar-Apr. Indian Dermatol Online J. 2025. PMID: 40125034 Free PMC article. No abstract available.
-
Entodermoscopy of Pediculosis capitis.JAAD Case Rep. 2022 Feb 15;22:70-71. doi: 10.1016/j.jdcr.2022.02.011. eCollection 2022 Apr. JAAD Case Rep. 2022. PMID: 35330983 Free PMC article. No abstract available.
-
Clinico-Dermoscopic Report of Molluscum Dermatitis: A Pearly Puzzle in Focus.Cureus. 2024 Dec 16;16(12):e75835. doi: 10.7759/cureus.75835. eCollection 2024 Dec. Cureus. 2024. PMID: 39822409 Free PMC article.
-
What's Bugging You: A Closer Look at the Crab Louse.Indian Dermatol Online J. 2022 Jan 24;13(1):143-144. doi: 10.4103/idoj.IDOJ_161_21. eCollection 2022 Jan-Feb. Indian Dermatol Online J. 2022. PMID: 35198491 Free PMC article. No abstract available.
References
-
- Sonthalia S, Errichetti E. Dermoscopy—not just for diagnosis and not just for dermatologists! Kathmandu Univ Med J (KUMJ) 2017;15:1–2. - PubMed
-
- Sonthalia S, Yumeen S, Kaliyadan F. Dermoscopy Overview and Extradiagnostic Applications. [Updated 2020 Aug 13]. In: StatPearls [Internet] Treasure Island (FL): StatPearls Publishing; 2020. Jan, - PubMed
-
- Scanni G, Bonifazi E. Viability of the head louse eggs in pediculosis capitis. A dermoscopy study. Eur J Pediat Dermatol. 2006;16:201–4.
Publication types
LinkOut - more resources
Full Text Sources
