

Case Reports
doi: 10.4103/idoj.IDOJ_568_20.
eCollection 2021 Mar-Apr.
The Puzzle of Papules Over Face and Extrafacial Areas: A Rare Case of Disseminated Idiopathic T-Cell Pseudolymphoma
Affiliations
- PMID: 33959532
- PMCID: PMC8088159
- DOI: 10.4103/idoj.IDOJ_568_20
Item in Clipboard
Case Reports
The Puzzle of Papules Over Face and Extrafacial Areas: A Rare Case of Disseminated Idiopathic T-Cell Pseudolymphoma
Indian Dermatol Online J.
.
Abstract
Papular lesions over face have a wide range of differential diagnoses. The clinical differentiation among these is difficult and often requires clinicopathological correlation. We hereby report the case of a 28 year old female presenting with numerous skin colored papular lesions over face, pinna and upper limbs.
Keywords: Cutaneous lymphoid hyperplasia; lichenoid pseudovesicular papular eruption on nose; lymphocytic infiltrate; lymphocytoma cutis; papules over nose.
Copyright: © 2021 Indian Dermatology Online Journal.
Conflict of interest statement
There are no conflicts of interest.
Figures

Multiple skin colored to erythematous, translucent, firm papules were present bilaterally symmetrical over nose, cheeks, and forehead

(a and b) Clinical image showing skin-colored papules present bilaterally over pinna, pre- and post-auricular areas. (c and d) Multiple erythematous and lichenoid papules over both forearms and dorsum of hands
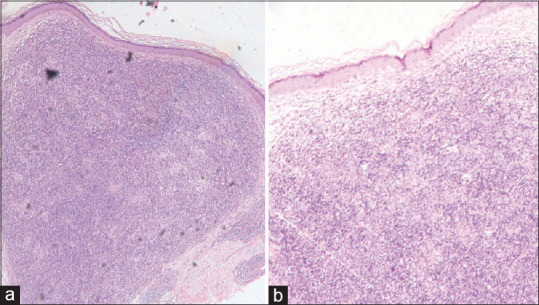
Histopathological image showing (a) Normal epidermis with clear subepidermal zone, and dense and diffuse lymphocytic infiltrate throughout the dermis (H and E, ×20). (b) Similar findings seen on higher magnification (×40)
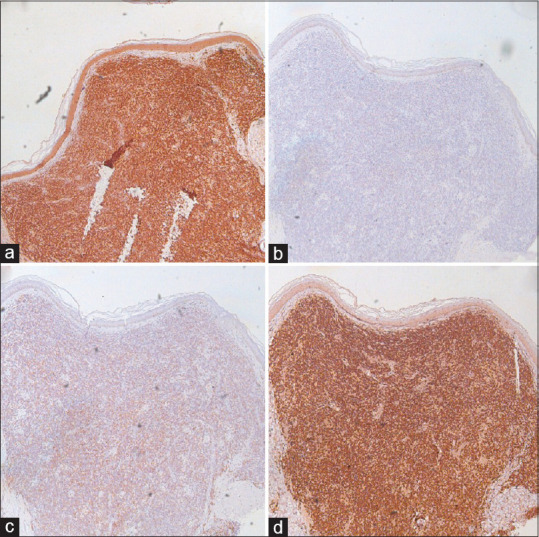
Immunohistochemistry staining for (a) CD3+ T cells, (b) CD4+ T cells, (c) CD5+ T cells, (d) CD8+ T cells showing infiltrate strongly positive for CD3+ and CD8+ T cells
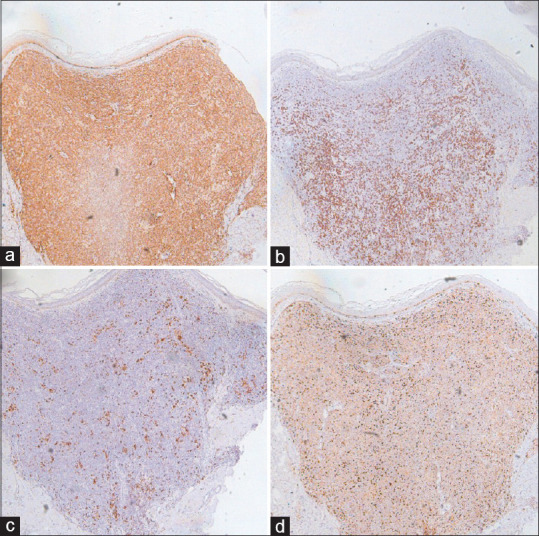
Immunohistochemistry staining for (a) bcl-2, (b) CD20+ B cells, (c) CD68+ histiocytes, (d) Ki-67 showing infiltrate weakly positive for CD20+ B cells and CD68+ histiocytes

Post treatment clinical image of face showing good response to treatment except few lesions over nose

Post treatment clinical images of (a and b) bilateral pinna, pre- and post-auricular areas, and (c and d) both upper limbs showing resolution of lesions
References
-
- Hussein MR. Cutaneous pseudolymphomas: Inflammatory reactive proliferations. Expert Rev Hematol. 2013;6:713–33. - PubMed
-
- Mitteldorf C, Kempf W. Cutaneous Pseudolymphoma. Surg Pathol Clin. 2017:10455–76. - PubMed
-
- Engin B, Songür A, Kutlubay Z, Serdaroğlu S. Lymphocytic infiltrations of face. Clin Dermatol. 2014;32:101–8. - PubMed
-
- Moulonguet I, Ghnassia M, Molina T, Fraitag S. Miliarial-type perifollicular B-cell pseudolymphoma (lymphocytoma cutis): A misleading eruption in two women. J Cutan Pathol. 2012;39:1016–21. - PubMed
-
- Thomas EA, Masih K, Sadiq S. Disseminated lymphadenosis benigna cutis. Indian J Dermatol. 2006;51:62–3.
Publication types
LinkOut - more resources
Full Text Sources
