

Multidisciplinary practice guidelines for the diagnosis, genetic counseling and treatment of pheochromocytomas and paragangliomas
- PMID: 33959901
- PMCID: PMC8390422
- DOI: 10.1007/s12094-021-02622-9
Multidisciplinary practice guidelines for the diagnosis, genetic counseling and treatment of pheochromocytomas and paragangliomas
Abstract
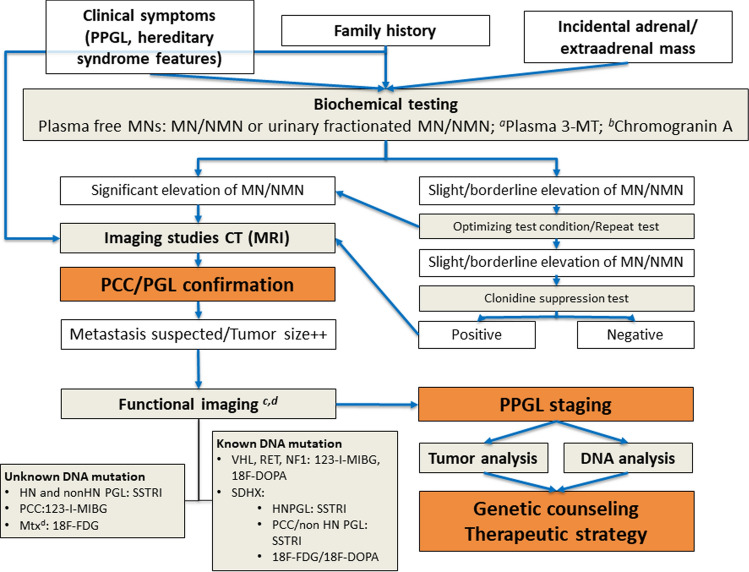
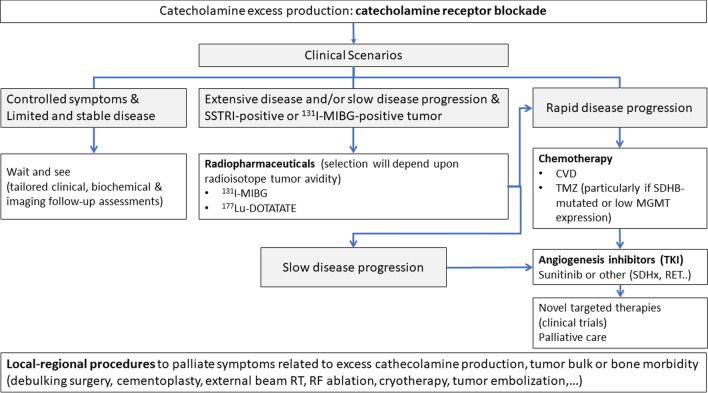
Pheochromocytomas and paragangliomas (PPGLs) are rare neuroendocrine tumors that arise from chromaffin cells of the adrenal medulla and the sympathetic/parasympathetic neural ganglia, respectively. The heterogeneity in its etiology makes PPGL diagnosis and treatment very complex. The aim of this article was to provide practical clinical guidelines for the diagnosis and treatment of PPGLs from a multidisciplinary perspective, with the involvement of the Spanish Societies of Endocrinology and Nutrition (SEEN), Medical Oncology (SEOM), Medical Radiology (SERAM), Nuclear Medicine and Molecular Imaging (SEMNIM), Otorhinolaryngology (SEORL), Pathology (SEAP), Radiation Oncology (SEOR), Surgery (AEC) and the Spanish National Cancer Research Center (CNIO). We will review the following topics: epidemiology; anatomy, pathology and molecular pathways; clinical presentation; hereditary predisposition syndromes and genetic counseling and testing; diagnostic procedures, including biochemical testing and imaging studies; treatment including catecholamine blockade, surgery, radiotherapy and radiometabolic therapy, systemic therapy, local ablative therapy and supportive care. Finally, we will provide follow-up recommendations.
Keywords: Diagnosis; Genetic counseling; Guidelines; Multidisciplinary; Paraganglioma; Pheochromocytoma; Treatment.
© 2021. The Author(s).
Conflict of interest statement
RGC has provided scientific advice and/or received honoraria or funding for continuous medical education from AAA, Advanz Pharma, Amgen, Bayer, BMS, HMP, Ipsen, Merck, Midatech Pharma, MSD, Novartis, PharmaMar, Pfizer, Pierre Fabre, Roche, Servier and Sanofi, and has received research support from Pfizer, MSD and BMS. EM-C has received honoraria for educational event from Medtronic Iberica S.A. CA-E has received payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events and support for attending meetings and/or travel from AAA (Advanced Accelerator Aplications, a Novartis Company), Novartis, Ipsen and Recordati. She has participated Participation on a Data Safety Monitoring Board or Advisory Board of Recordati. She has received medical writing services from Ipsen. FAH has provided scientific advice and/or received honoraria or funding for continuous medical education from Ipsen, Novartis and Pfizer. FMT, MM-C, MR, IT, MA, MRB-C and CF-A have no conflicts of interest to declare.
Figures
References
-
- Leung AA, Pasieka JL, Hyrcza MD, Pacaud D, Dong Y, Boyd JM, et al. Epidemiology of pheochromocytoma and paraganglioma: population-based cohort study. Eur J Endocrinol. 2021;184:19–28. - PubMed
-
- Rodriguez-Cuevas H, Lau I, Rodriguez HP. High-altitude paragangliomas diagnostic and therapeutic considerations. Cancer. 1986;57:672–676. - PubMed
-
- Berends AMA, Buitenwerf E, de Krijger RR, Veeger N, van der Horst-Schrivers ANA, Links TP, et al. Incidence of pheochromocytoma and sympathetic paraganglioma in the Netherlands: a nationwide study and systematic review. Eur J Intern Med. 2018;51:68–73. - PubMed
-
- Lack EE, Cubilla AL, Woodruff JM, Farr HW. Paragangliomas of the head and neck region: a clinical study of 69 patients. Cancer. 1977;39:397–409. - PubMed
-
- Lloyd RV, Osamura YR, Kloppel G, Rosai J. WHO classification of tumours of endocrine organs. Geneva: WHO Press; 2017.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
