

Effect of exercise on cardiometabolic health of adults with overweight or obesity: Focus on blood pressure, insulin resistance, and intrahepatic fat-A systematic review and meta-analysis
- PMID: 33960110
- PMCID: PMC8365642
- DOI: 10.1111/obr.13269
Effect of exercise on cardiometabolic health of adults with overweight or obesity: Focus on blood pressure, insulin resistance, and intrahepatic fat-A systematic review and meta-analysis
Abstract
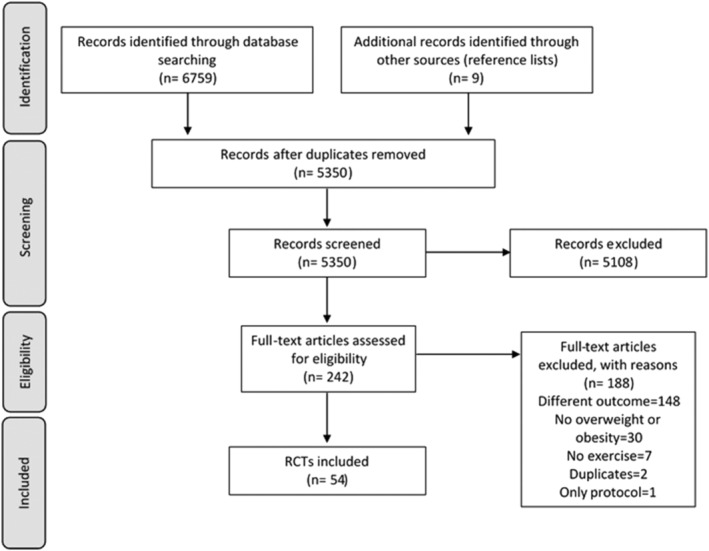
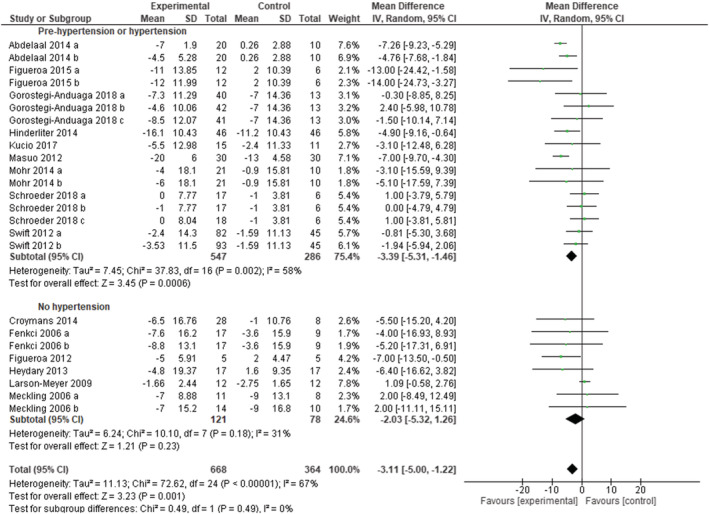
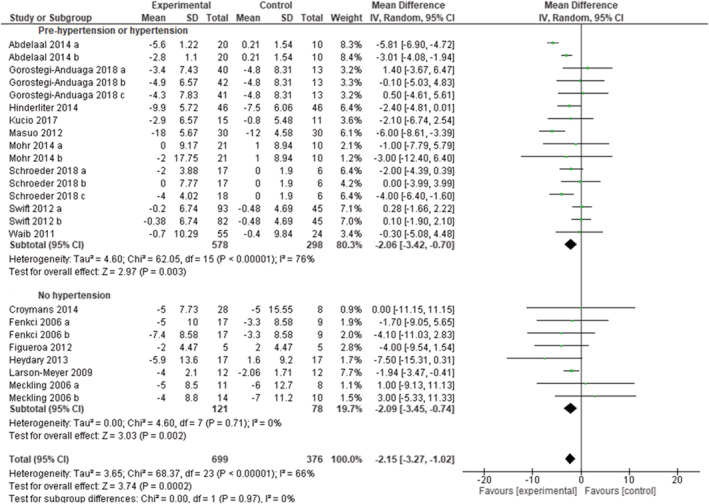
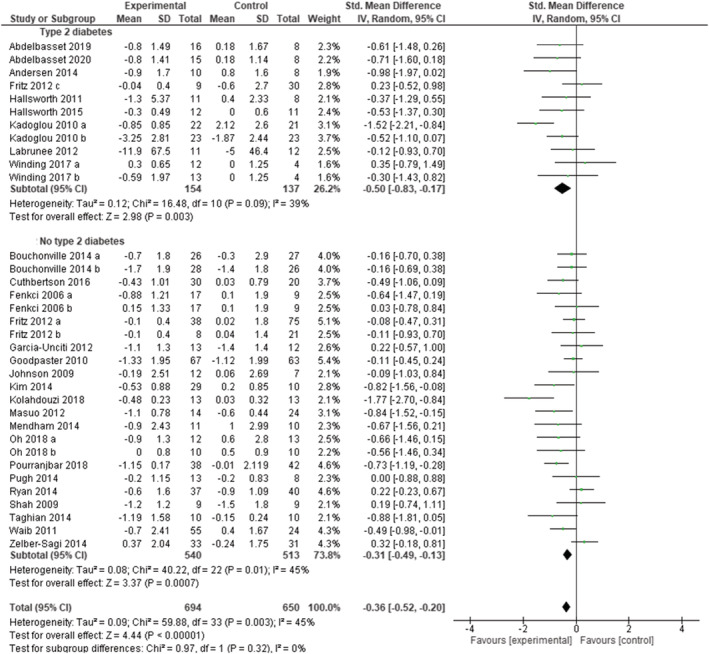
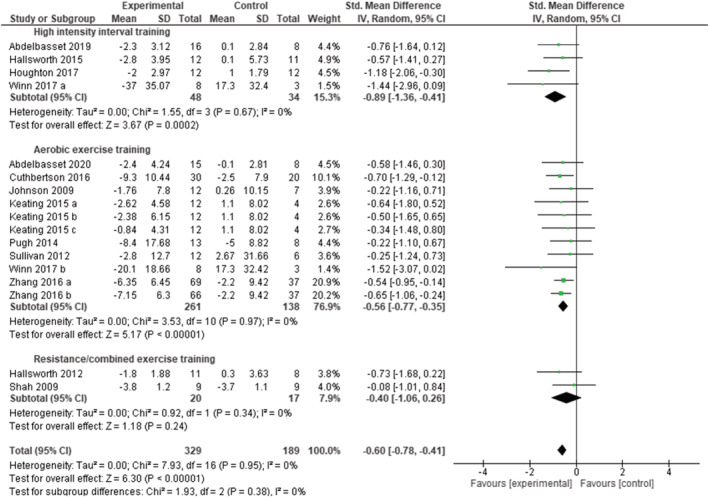
This systematic review examined the impact of exercise intervention programs on selected cardiometabolic health indicators in adults with overweight or obesity. Three electronic databases were explored for randomized controlled trials (RCTs) that included adults with overweight or obesity and provided exercise-training interventions. Effects on blood pressure, insulin resistance (homeostasis model of insulin resistance, HOMA-IR), and magnetic resonance measures of intrahepatic fat in exercise versus control groups were analyzed using random effects meta-analyses. Fifty-four articles matched inclusion criteria. Exercise training reduced systolic and diastolic blood pressure (mean difference, MD = -2.95 mmHg [95% CI -4.22, -1.68], p < 0.00001, I2 = 63% and MD = -1.93 mmHg [95% CI -2.73, -1.13], p < 0.00001, I2 = 54%, 60 and 58 study arms, respectively). Systolic and diastolic blood pressure decreased also when considering only subjects with hypertension. Exercise training significantly decreased HOMA-IR (standardized mean difference, SMD = -0.34 [-0.49, -0.18], p < 0.0001, I2 = 48%, 37 study arms), with higher effect size in subgroup of patients with type 2 diabetes (SMD = -0.50 [95% CI: -0.83, -0.17], p = 0.003, I2 = 39%). Intrahepatic fat decreased significantly after exercise interventions (SMD = -0.59 [95% CI: -0.78, -0.41], p < 0.00001, I2 = 0%), with a larger effect size after high-intensity interval training. In conclusion, exercise training is effective in improving cardiometabolic health in adults with overweight or obesity also when living with comorbitidies.
Keywords: NAFLD; hypertension; insulin resistance; morbid obesity; physical activity; type 2 diabetes.
© 2021 The Authors. Obesity Reviews published by John Wiley & Sons Ltd on behalf of World Obesity Federation.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi MBM, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur Heart J. 2018;39(33):3021‐3104. 10.1093/eurheartj/ehy339 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
