

Status epilepticus and diabetes ketoacidosis: uncommon clinical presentations of acromegaly
- PMID: 33960324
- PMCID: PMC8185527
- DOI: 10.1530/EDM-20-0156
Status epilepticus and diabetes ketoacidosis: uncommon clinical presentations of acromegaly
Abstract
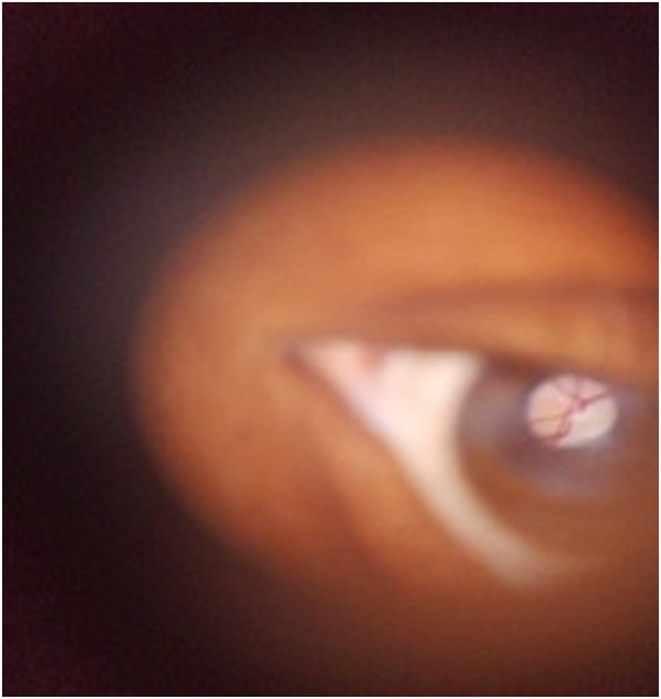
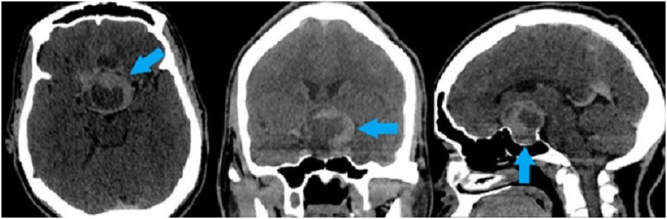
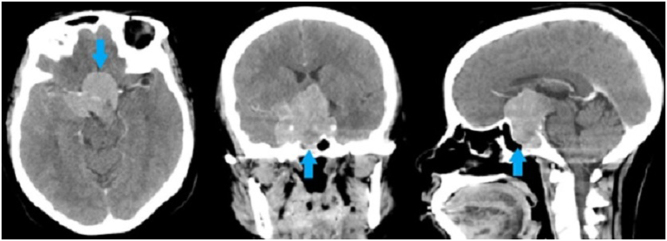
Summary: Acromegaly is a rare disease caused by hypersecretion of the growth hormone (GH). Most cases are caused by either pituitary microadenoma or macroadenoma. The GH producing tumors present with clinical manifestations of acromegaly due to excessive GH secretion or symptoms resulting from mass effects of the enlarging tumor. The physical changes are usually slow and, therefore, recognition of the disease is delayed. These adenomas are never malignant but can have significant morbidity and mortality. A subgroup of patients with acromegaly present with severe hyperglycemia resulting in diabetic ketoacidosis (DKA) which requires insulin. Rarely are pituitary tumors responsible for generalized convulsions except when they are too large. We hereby present two cases, the first is that of a 26-year-old female who presented with new onset status epilepticus, DKA with a 1-year history of diabetes mellitus (DM). On examination, she had clinical features of acromegaly. The second case is that of a 34-year-old female who presented with new onset status epilepticus, hyperglycemia with a history of recently diagnosed DM, and features of gigantism. In both cases, their diagnosis was confirmed by elevated serum GH and later by elevated insulin-like growth factor type 1 levels, and CT of the head demonstrating large pituitary macroadenoma. The importance of clinical history and examination, as well as investigations is vital in the recognition of acromegaly. The prognosis of acromegalic patients depends on early clinical recognition and tumor size reduction by either medical or surgical therapy.
Learning points: Conditions such as status epilepticus and DKA may be clinical presentations in patients presenting with acromegaly. Seizures are rare in people with pituitary adenoma and typically occur when the tumor invades the suprasellar area due to mass effect on the brain. This article shows how best we were able to manage the acromegaly complications in a low resource setting. Hyperprolactinemia in acromegaly may be due to disruption of the normal dopaminergic inhibition of prolactin secretion due to mass effect of the macroadenoma, and around 25% of GH-secreting adenomas co-secrete prolactin.
Figures

Similar articles
-
Thyrotoxicosis with absence of clinical features of acromegaly in a TSH- and GH-secreting, invasive pituitary macroadenoma.Endocrinol Diabetes Metab Case Rep. 2015;2015:140070. doi: 10.1530/EDM-14-0070. Epub 2015 Jan 1. Endocrinol Diabetes Metab Case Rep. 2015. PMID: 25614823 Free PMC article.
-
Neuroendocrine tumors secreting growth hormone-releasing hormone: Pathophysiological and clinical aspects.Pituitary. 2006;9(3):221-9. doi: 10.1007/s11102-006-0267-0. Pituitary. 2006. PMID: 17036195 Review.
-
Acromegaly: report of two patients with an unusual presentation.Neth J Med. 1999 Apr;54(4):163-6. doi: 10.1016/s0300-2977(99)00003-0. Neth J Med. 1999. PMID: 10218386
-
Diagnosis and treatment of pituitary adenomas.Minerva Endocrinol. 2004 Dec;29(4):241-75. Minerva Endocrinol. 2004. PMID: 15765032 Review.
-
Ectopic secretion of growth hormone-releasing hormone (GHRH) in neuroendocrine tumors: relevant clinical aspects.Ann Oncol. 2001;12 Suppl 2:S89-94. doi: 10.1093/annonc/12.suppl_2.s89. Ann Oncol. 2001. PMID: 11762359 Review.
Cited by
-
Dietary Influence on Drug Efficacy: A Comprehensive Review of Ketogenic Diet-Pharmacotherapy Interactions.Nutrients. 2024 Apr 19;16(8):1213. doi: 10.3390/nu16081213. Nutrients. 2024. PMID: 38674903 Free PMC article. Review.
-
Acromegaly Initially Presenting with Severe Infectious Diseases: A Case Report.JMA J. 2022 Jan 17;5(1):161-166. doi: 10.31662/jmaj.2021-0150. Epub 2021 Dec 24. JMA J. 2022. PMID: 35224284 Free PMC article.
References
-
- Caron P, Brue T, Raverot G, Tabarin A, Cailleux A, Delemer B, Renoult PP, Houchard A, Elaraki F, Chanson P.Signs and symptoms of acromegaly at diagnosis: the physician’s and the patient’s perspectives in the ACRO-POLIS study. Endocrine 2019. 63 120–129. (10.1007/s12020-018-1764-4) - DOI - PMC - PubMed
-
- Møller N, Schmitz O, Jøorgensen JO, Astrup J, Bak JF, Christensen SE, Alberti KG, Weeke J.Basal- and insulin-stimulated substrate metabolism in patients with active acromegaly before and after adenomectomy. Journal of Clinical Endocrinology and Metabolism 1992. 74 1012–1019. (10.1210/jcem.74.5.1569148) - DOI - PubMed
-
- Fieffe S, Morange I, Petrossians P, Chanson P, Rohmer V, Cortet C, Borson-Chazot F, Brue T, Delemer B.French Acromegaly Registry. Diabetes in acromegaly, prevalence, risk factors, and evolution: data from the French Acromegaly Registry. European Journal of Endocrinology 2011. 164 877–884. (10.1530/EJE-10-1050) - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
