

Artificial intelligence in oncology: Path to implementation
- PMID: 33960708
- PMCID: PMC8209596
- DOI: 10.1002/cam4.3935
Artificial intelligence in oncology: Path to implementation
Abstract
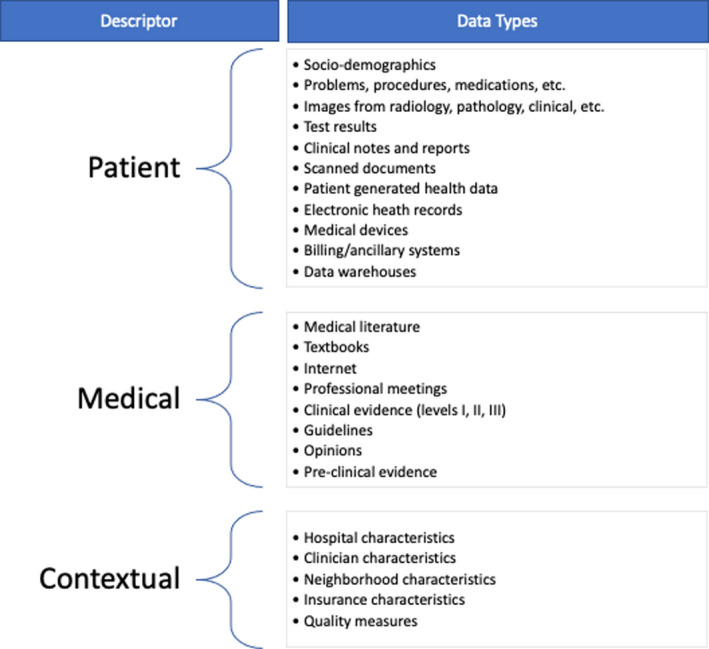
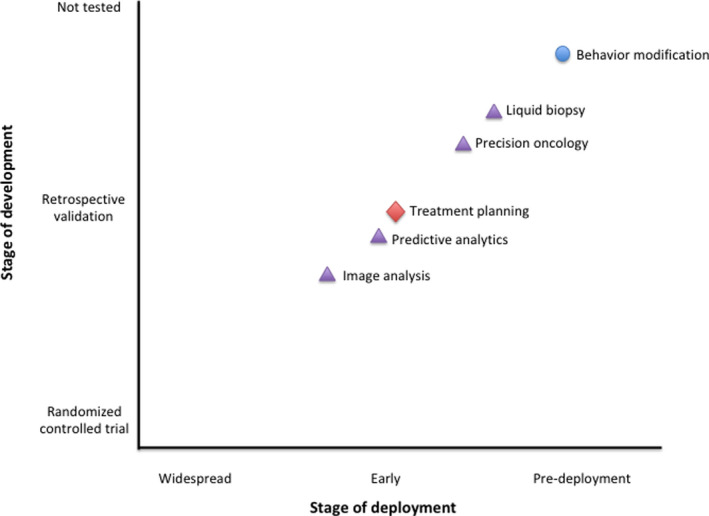
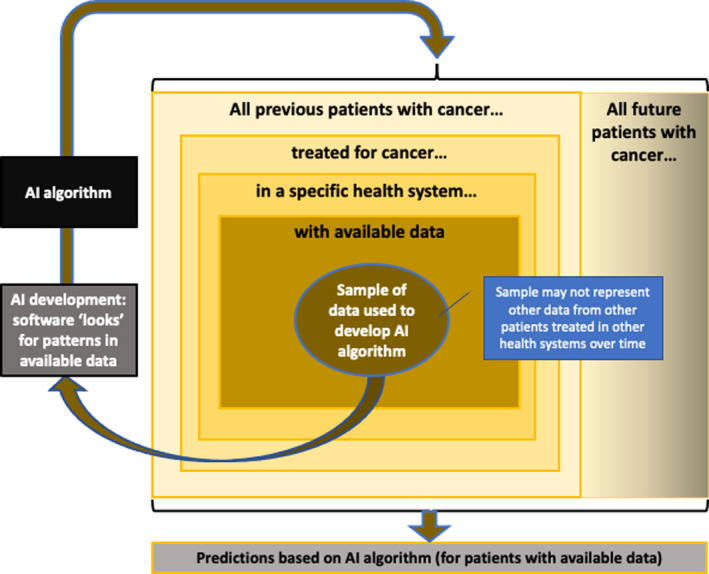
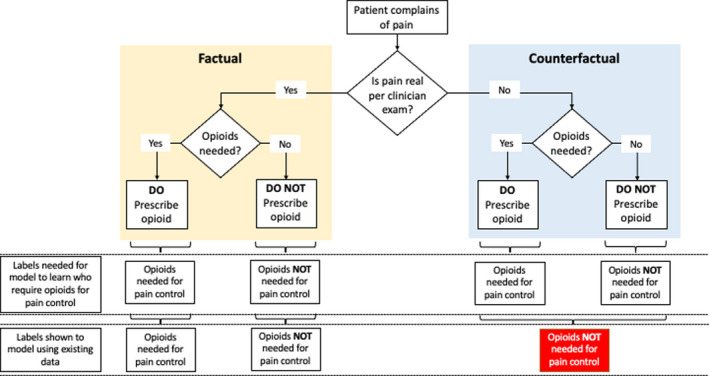
In recent years, the field of artificial intelligence (AI) in oncology has grown exponentially. AI solutions have been developed to tackle a variety of cancer-related challenges. Medical institutions, hospital systems, and technology companies are developing AI tools aimed at supporting clinical decision making, increasing access to cancer care, and improving clinical efficiency while delivering safe, high-value oncology care. AI in oncology has demonstrated accurate technical performance in image analysis, predictive analytics, and precision oncology delivery. Yet, adoption of AI tools is not widespread, and the impact of AI on patient outcomes remains uncertain. Major barriers for AI implementation in oncology include biased and heterogeneous data, data management and collection burdens, a lack of standardized research reporting, insufficient clinical validation, workflow and user-design challenges, outdated regulatory and legal frameworks, and dynamic knowledge and data. Concrete actions that major stakeholders can take to overcome barriers to AI implementation in oncology include training and educating the oncology workforce in AI; standardizing data, model validation methods, and legal and safety regulations; funding and conducting future research; and developing, studying, and deploying AI tools through multidisciplinary collaboration.
Keywords: artificial intelligence; deep learning; machine learning; oncology.
© 2021 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
Except I.S.C. and M.H., all other coauthors have declared no conflict of interests.
Figures
References
-
- Bates DW, Auerbach A, Schulam P, Wright A, Saria S. Reporting and implementing interventions involving machine learning and artificial intelligence. Ann Intern Med. 2020;172:S137‐S144. - PubMed
-
- Esteva A, Robicquet A, Ramsundar B, et al. A guide to deep learning in healthcare. Nat Med. 2019;25:24‐29. - PubMed
-
- What to expect from AI in oncology. Nat Rev Clin Oncol. 2019;16:655. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;2020(70):7‐30. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
