

A series of COVID-19 autopsies with clinical and pathologic comparisons to both seasonal and pandemic influenza
- PMID: 33960723
- PMCID: PMC8239851
- DOI: 10.1002/cjp2.220
A series of COVID-19 autopsies with clinical and pathologic comparisons to both seasonal and pandemic influenza
Abstract
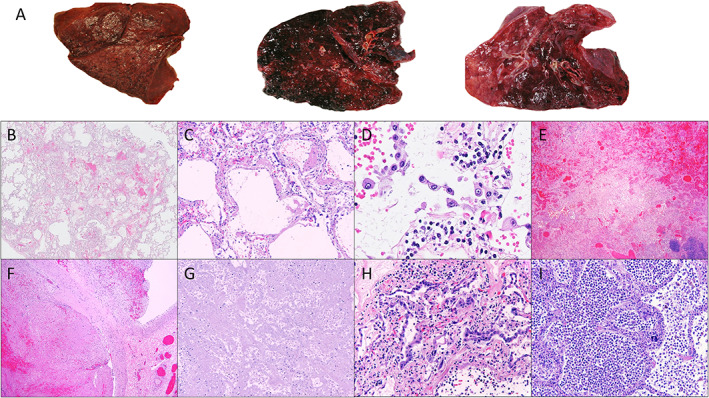
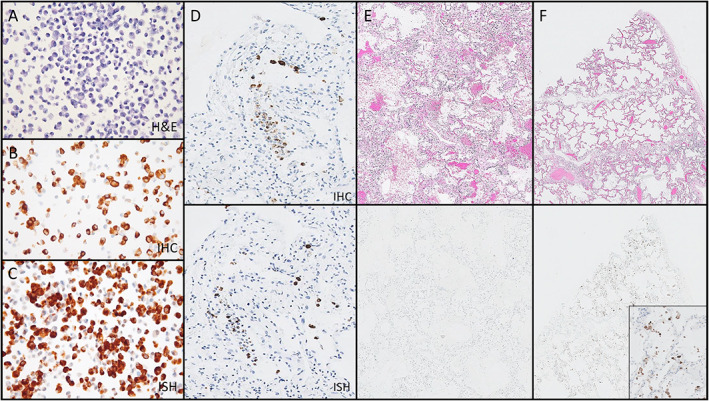
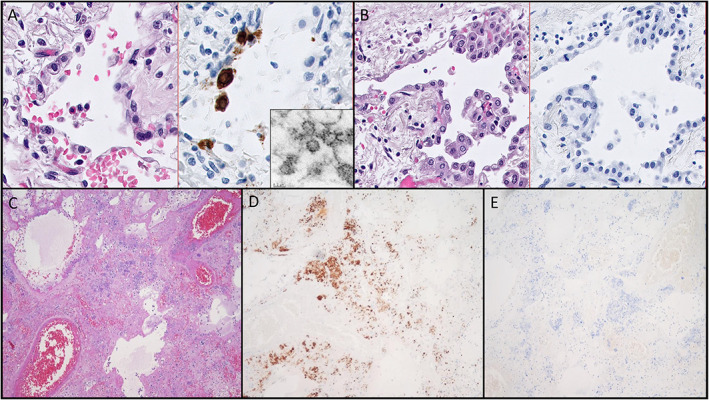
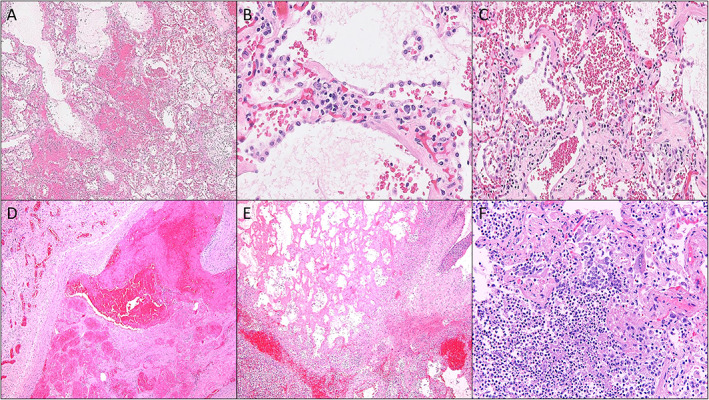
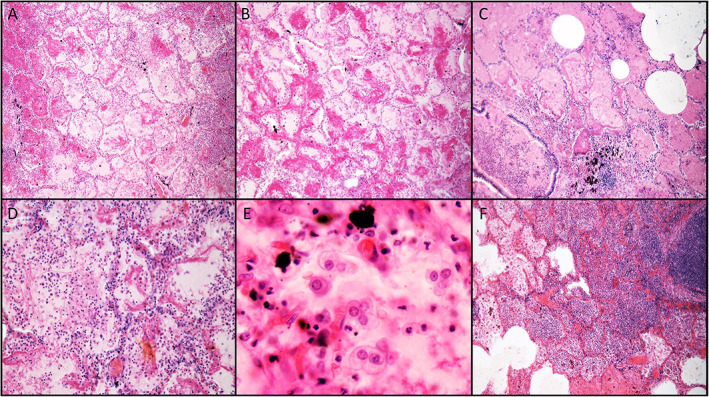
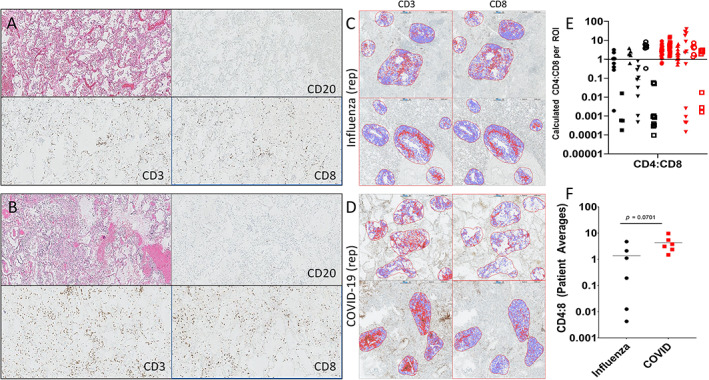
Autopsies of patients who have died from COVID-19 have been crucial in delineating patterns of injury associated with SARS-CoV-2 infection. Despite their utility, comprehensive autopsy studies are somewhat lacking relative to the global burden of disease, and very few comprehensive studies contextualize the findings to other fatal viral infections. We developed a novel autopsy protocol in order to perform postmortem examinations on victims of COVID-19 and herein describe detailed clinical information, gross findings, and histologic features observed in the first 16 complete COVID-19 autopsies. We also critically evaluated the role of ancillary studies used to establish a diagnosis of COVID-19 at autopsy, including immunohistochemistry (IHC), in situ hybridization (ISH), and electron microscopy (EM). IHC and ISH targeting SARS-CoV-2 were comparable in terms of the location and number of infected cells in lung tissue; however, nonspecific staining of bacteria was seen occasionally with IHC. EM was unrevealing in blindly sampled tissues. We then compared the clinical and histologic features present in this series to six archival cases of fatal seasonal influenza and six archival cases of pandemic influenza from the fourth wave of the 'Spanish Flu' in the winter of 1920. In addition to routine histology, the inflammatory infiltrates in the lungs of COVID-19 and seasonal influenza victims were compared using quantitative IHC. Our results demonstrate that the clinical and histologic features of COVID-19 are similar to those seen in fatal cases of influenza, and the two diseases tend to overlap histologically. There was no significant difference in the composition of the inflammatory infiltrate in COVID-19 and influenza at sites of acute lung injury at the time of autopsy. Our study underscores the relatively nonspecific clinical features and pathologic changes shared between severe cases of COVID-19 and influenza, while also providing important caveats to ancillary methods of viral detection.
Keywords: COVID-19; autopsy; diffuse alveolar damage; influenza; viral pneumonia; viral sepsis.
© 2021 The Authors. The Journal of Pathology: Clinical Research published by The Pathological Society of Great Britain and Ireland & John Wiley & Sons, Ltd.
Figures
Similar articles
-
Comparison of RNA In Situ Hybridization and Immunohistochemistry Techniques for the Detection and Localization of SARS-CoV-2 in Human Tissues.Am J Surg Pathol. 2021 Jan;45(1):14-24. doi: 10.1097/PAS.0000000000001563. Am J Surg Pathol. 2021. PMID: 32826529
-
Higher prevalence of pulmonary macrothrombi in SARS-CoV-2 than in influenza A: autopsy results from 'Spanish flu' 1918/1919 in Switzerland to Coronavirus disease 2019.J Pathol Clin Res. 2021 Mar;7(2):135-143. doi: 10.1002/cjp2.189. Epub 2020 Nov 13. J Pathol Clin Res. 2021. PMID: 33185036 Free PMC article.
-
Tissue-based SARS-CoV-2 detection in fatal COVID-19 infections: Sustained direct viral-induced damage is not necessary to drive disease progression.Hum Pathol. 2021 Aug;114:110-119. doi: 10.1016/j.humpath.2021.04.012. Epub 2021 May 4. Hum Pathol. 2021. PMID: 33961839 Free PMC article.
-
Autopsies in pandemics - a perspective on barriers and benefits. Is it time for a revival?APMIS. 2021 Jul;129(7):324-339. doi: 10.1111/apm.13111. Epub 2021 Mar 1. APMIS. 2021. PMID: 33645838 Free PMC article. Review.
-
Lung Histopathology in Coronavirus Disease 2019 as Compared With Severe Acute Respiratory Sydrome and H1N1 Influenza: A Systematic Review.Chest. 2021 Jan;159(1):73-84. doi: 10.1016/j.chest.2020.09.259. Epub 2020 Oct 7. Chest. 2021. PMID: 33038391 Free PMC article.
Cited by
-
SARS-CoV-2-Infection (COVID-19): Clinical Course, Viral Acute Respiratory Distress Syndrome (ARDS) and Cause(s) of Death.Med Sci (Basel). 2022 Oct 10;10(4):58. doi: 10.3390/medsci10040058. Med Sci (Basel). 2022. PMID: 36278528 Free PMC article. Review.
-
Postmortem Cardiopulmonary Pathology in Patients with COVID-19 Infection: Single-Center Report of 12 Autopsies from Lausanne, Switzerland.Diagnostics (Basel). 2021 Jul 28;11(8):1357. doi: 10.3390/diagnostics11081357. Diagnostics (Basel). 2021. PMID: 34441292 Free PMC article.
-
Prospective and Longitudinal Analysis of Lymphocyte Subpopulations in SARS-CoV-2 Positive and Negative Pneumonia: Potential Role of Decreased Naïve CD8+ in COVID-19 Patients.Viruses. 2024 Dec 30;17(1):41. doi: 10.3390/v17010041. Viruses. 2024. PMID: 39861830 Free PMC article.
-
Autopsy findings in COVID-19 infection-related death: a systematic review.Egypt J Forensic Sci. 2022;12(1):22. doi: 10.1186/s41935-022-00280-8. Epub 2022 May 10. Egypt J Forensic Sci. 2022. PMID: 35573158 Free PMC article. Review.
-
Increase of mast cells in COVID-19 pneumonia may contribute to pulmonary fibrosis and thrombosis.Histopathology. 2023 Feb;82(3):407-419. doi: 10.1111/his.14838. Epub 2022 Nov 27. Histopathology. 2023. PMID: 36366933 Free PMC article.
References
-
- World Health Organization . Coronavirus disease (COVID‐2019) situation reports. [Accessed 29 March 2021]. Available from: https://www.who.int/publications/m/item/weekly-epidemiological-update-on...
-
- Hanley B, Lucas SB, Youd E, et al. Autopsy in suspected COVID‐19 cases. J Clin Pathol 2020; 73: 239–242. - PubMed
-
- Center for Disease Control . COVID‐19 post‐mortem guidance. [Updated 22 November 2020, accessed 29 March 2021]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-postmortem-specim...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
