

Heart failure related to adult congenital heart disease: prevalence, outcome and risk factors
- PMID: 33960724
- PMCID: PMC8318399
- DOI: 10.1002/ehf2.13378
Heart failure related to adult congenital heart disease: prevalence, outcome and risk factors
Abstract
Aims: Information on the prevalence, outcome and factors associated with heart failure in patients with adult congenital heart disease (CHD) (ACHD-HF) is lacking. We aimed at assessing the prevalence and outcome of ACHD-HF, the variables associated with ACHD-HF, and the differences between major anatomical/pathophysiological ACHD subgroups.
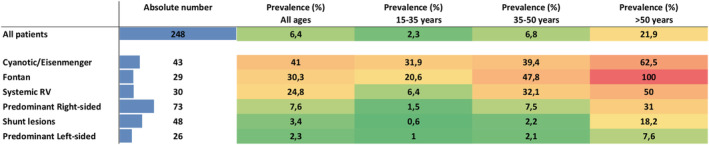
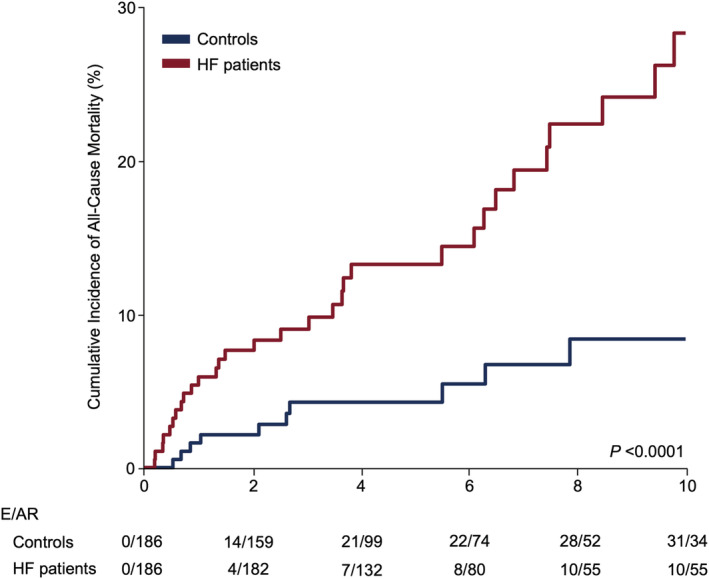
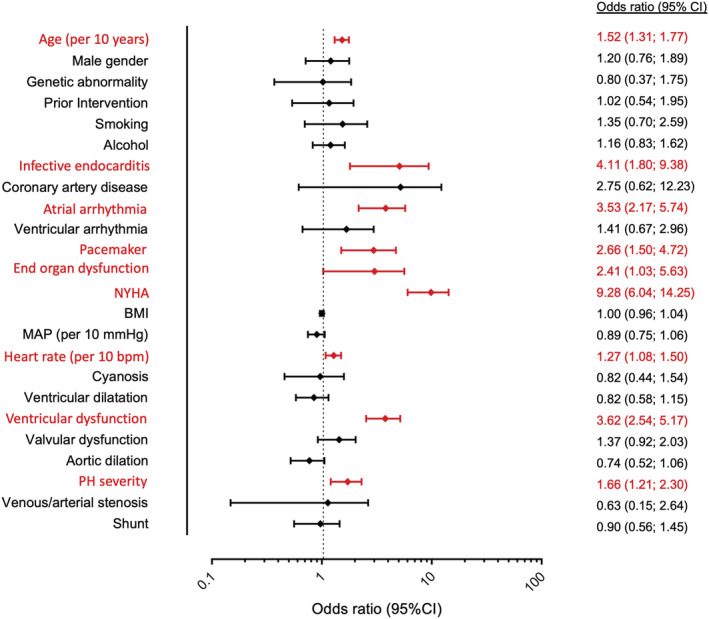
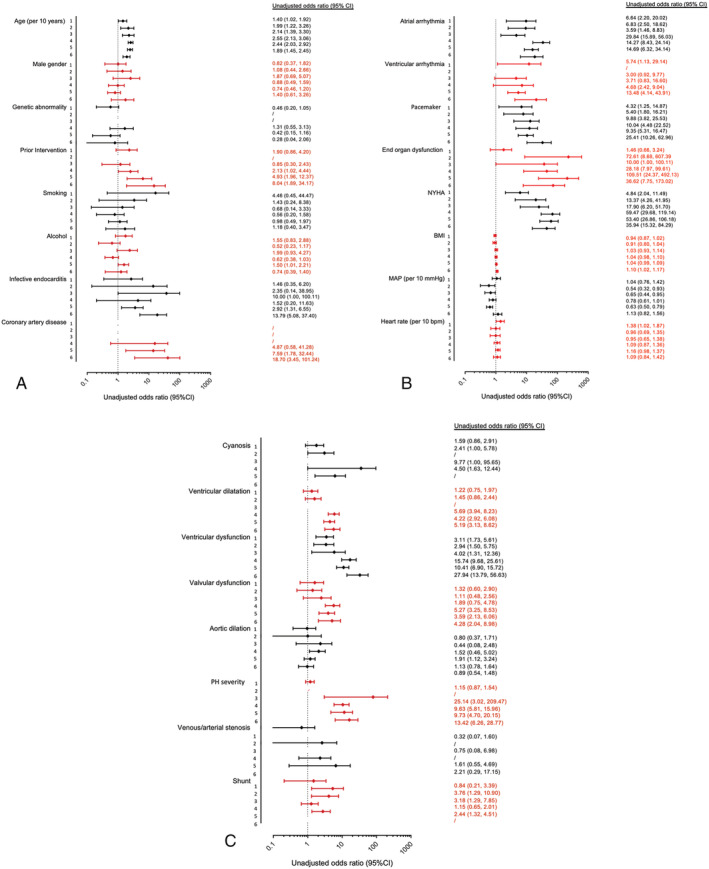
Methods and results: We included 3905 patients (age 35.4 ± 13.2 years) under active follow-up in our institution (last visit >2010). Outcome of ACHD-HF cases was compared with sex- and age-matched cases. Univariable and multivariable binary logistic regression with ACHD-HF diagnosis as a dependent variable was performed. Overall prevalence of ACHD-HF was 6.4% (mean age 49.5 ± 16.7 years), but was higher in patients with cyanotic CHD (41%), Fontan circulation (30%), and a systemic right ventricle (25%). All-cause mortality was higher in ACHD-HF cases when compared with controls (mortality rate ratio 4.67 (2.36-9.27); P = 0.0001). In multivariable logistic regression analysis, age at latest follow-up [per 10 years; odds ratio (OR) 1.52; 95% confidence interval (CI) 1.31-1.77], infective endocarditis (OR 4.11; 95%CI 1.80-9.38), history of atrial arrhythmia (OR 3.52; 95%CI 2.17-5.74), pacemaker implantation (OR 2.66; 95% CI 1.50-4.72), end-organ dysfunction (OR 2.41; 95% CI 1.03-5.63), New York Heart Association class (OR 9.28; 95% CI 6.04-14.25), heart rate (per 10 bpm; OR 1.27; 95% CI 1.08-1.50), ventricular dysfunction (OR 3.62; 95% CI 2.54-5.17), and pulmonary hypertension severity (OR 1.66; 95% CI 1.21-2.30) were independently related to the presence of ACHD-HF. Some variables (age, atrial arrhythmia, pacemaker, New York Heart Association, and ventricular dysfunction) were related to ACHD-HF in all anatomical/physiological subgroups, whereas others were not.
Conclusions: ACHD-HF is prevalent especially in complex CHD and is associated with poor prognosis. Our data provide insight in the factors related to ACHD-HF including differences between specific anatomical and physiological subgroups.
Keywords: ACHD; All-cause mortality; Congenital; Heart failure.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
No conflicts of interest.
Figures
References
-
- Moons P, Bovijn L, Budts W, Belmans A, Gewillig M. Temporal trends in survival to adulthood among patients born with congenital heart disease from 1970 to 1992 in Belgium. Circulation 2010; 122: 2264–2272. - PubMed
-
- Baumgartner H. Geriatric congenital heart disease: a new challenge in the care of adults with congenital heart disease? Eur Heart J 2014; 35: 683–685. - PubMed
-
- Tutarel O, Kempny A, Alonso‐Gonzalez R, Jabbour R, Li W, Uebing A, Dimopoulos K, Swan L, Gatzoulis MA, Diller GP. Congenital heart disease beyond the age of 60: emergence of a new population with high resource utilization, high morbidity, and high mortality. Eur Heart J 2014; 35: 725–732. - PubMed
-
- Bruaene A, Van De Hickey EJ, Kovacs AH, Crean AM, Wald RM, Silversides CK, Redington AN, Ross HJ, Alba AC, Billia F, Nair K, Benson L, Horlick E, Osten M, Colman J, Heggie J, Oechslin EN, Roche SL. Phenotype, management and predictors of outcome in a large cohort of adult congenital heart disease patients with heart failure. Int J Cardiol 2018; 252: 80–87. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
