

Colchicine and the heart
- PMID: 33961006
- PMCID: PMC8294843
- DOI: 10.1093/eurheartj/ehab221
Colchicine and the heart
Abstract
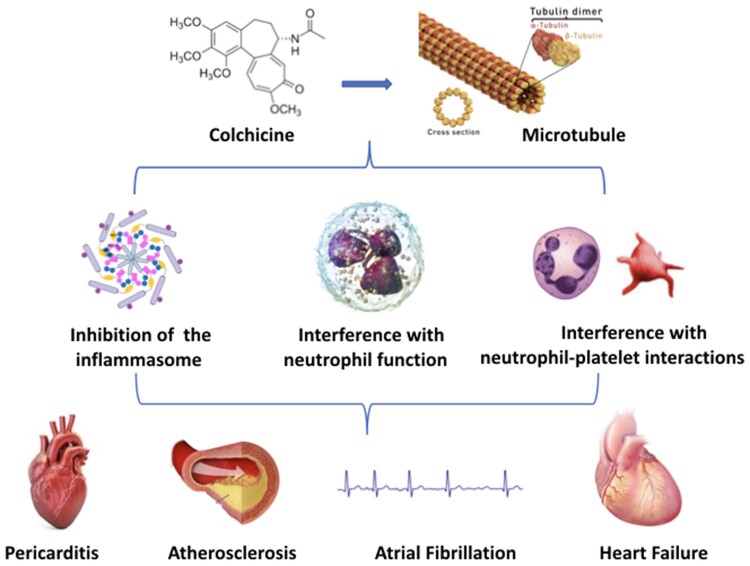
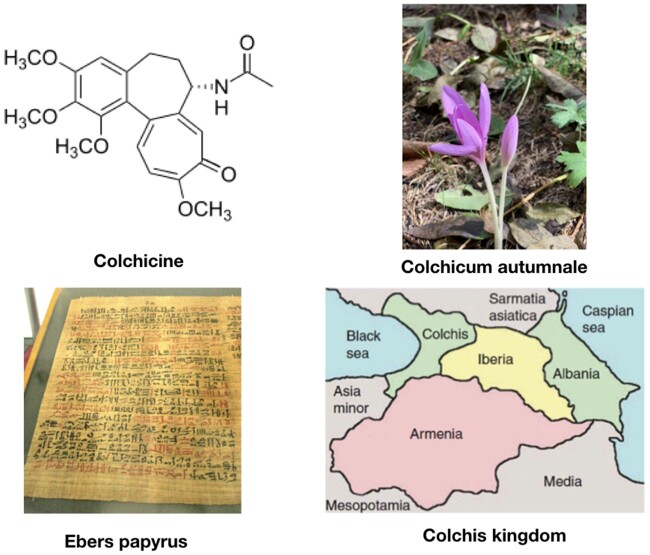
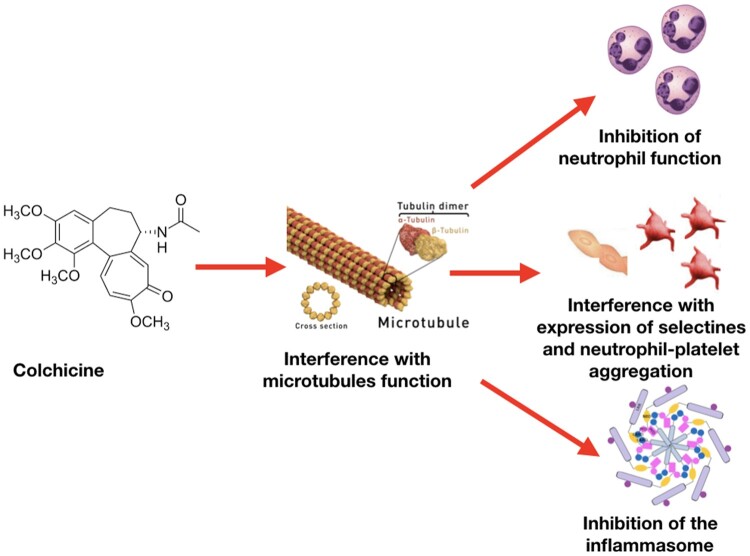
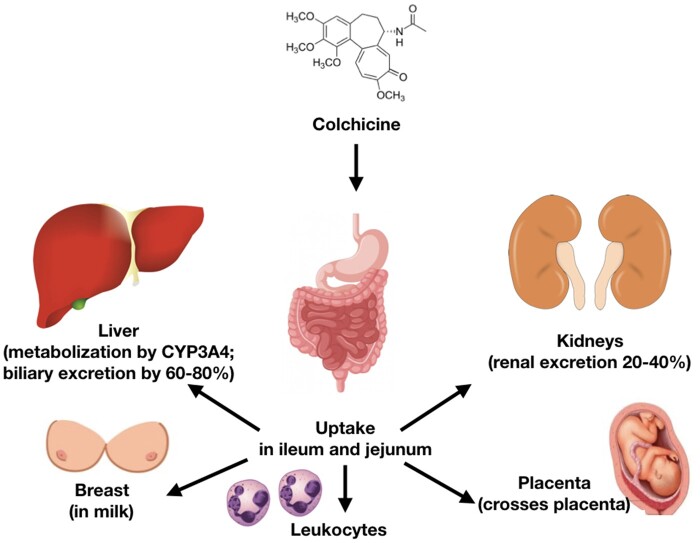
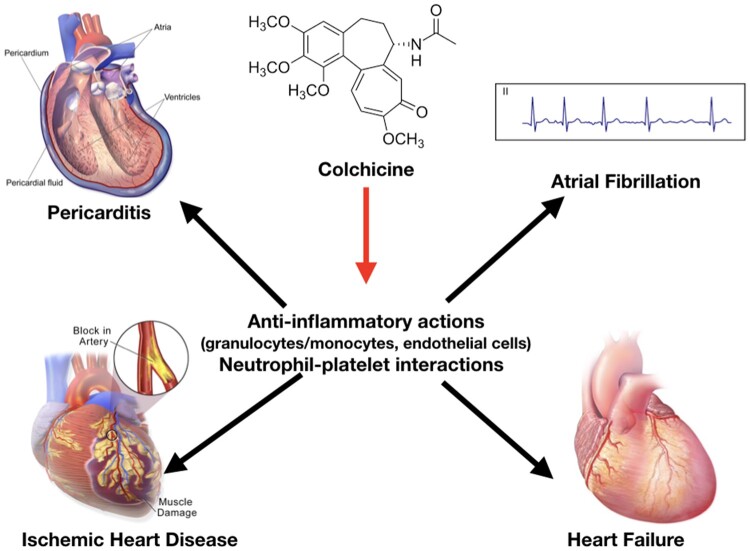
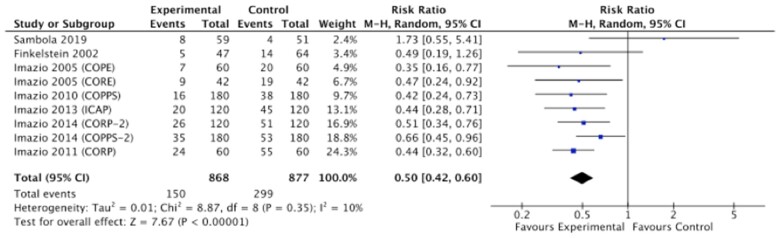
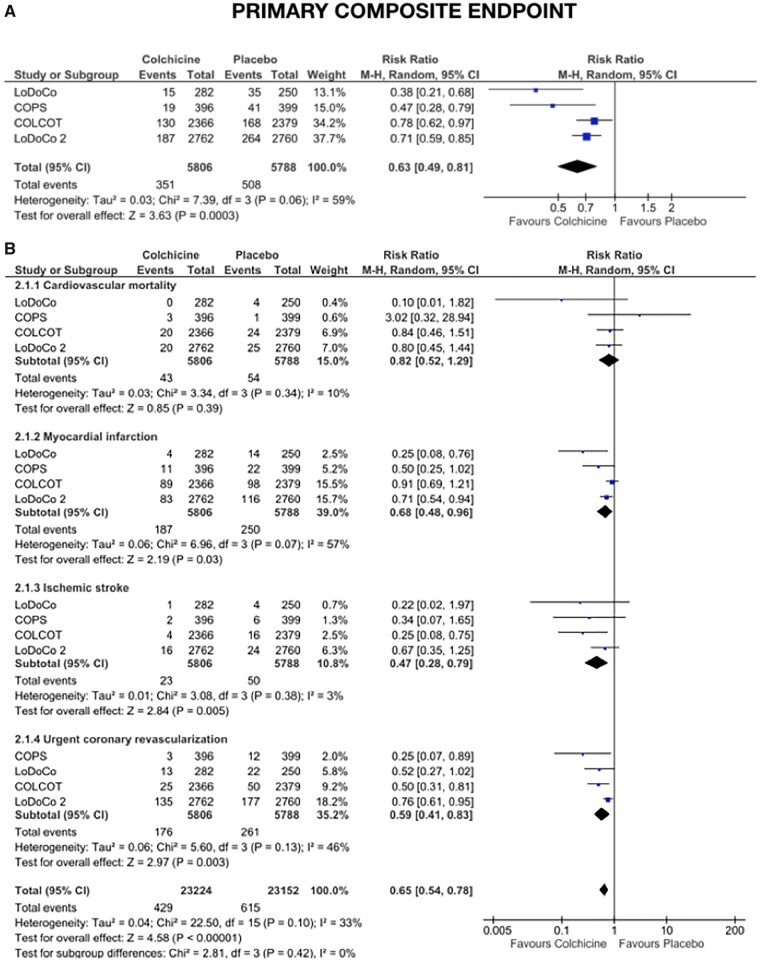
Colchicine is a unique, sophisticated anti-inflammatory agent that has been used for decades for the prevention of acute inflammatory flares in gout and familial Mediterranean fever. In recent years, clinical trials have demonstrated its potential in a range of cardiovascular (CV) conditions. Colchicine is avidly taken up by leucocytes, and its ability to bind to tubulin and interfere with microtubular function affects the expression of cytokines and interleukins, and the ability of neutrophils to marginate, ingress, aggregate, express superoxide, release neutrophil extracellular traps, and interact with platelets. In patients with acute and recurrent pericarditis, clinical trials in >1600 patients have consistently shown that colchicine halves the risk of recurrence [relative risk (RR) 0.50, 95% confidence interval (CI) 0.42-0.60]. In patients with acute and chronic coronary syndromes, multicentre randomized controlled trials in >11 000 patients followed for up to 5 years demonstrated that colchicine may reduce the risk of CV death, myocardial infarction, ischaemic stroke and ischaemia-driven revascularization by >30% (RR 0.63, 95% CI 0.49-0.81). The use of colchicine at doses of 0.5-1.0 mg daily in CV trials has proved safe. Early gastrointestinal intolerance limits its use in ∼10% of patients; however, ∼90% of patients tolerate it well over the long term. Despite isolated case reports, clinically relevant drug interactions with moderate to strong CYP3A4 inhibitors/competitors or P-glycoprotein inhibitors/competitors are rare if this dosage of colchicine is used in the absence of advanced renal or liver disease. The aim of this review is to summarize the contemporary data supporting the efficacy and safety of colchicine in patients with CV disease.
Keywords: Acute coronary syndrome; Atrial fibrillation; Chronic coronary syndrome; Colchicine; Coronary artery disease; Heart failure; Inflammasome; Pericarditis.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Nerlekar N, Beale A, Harper RW. Colchicine—a short history of an ancient drug. Med J Aust 2014;201:687–688. - PubMed
-
- Bayes-Genis A, Adler Y, de Luna AB, Imazio M. Colchicine in pericarditis. Eur Heart J 2017;38:1706–1709. - PubMed
-
- Dalbeth N, Lauterio TJ, Wolfe HR. Mechanism of action of colchicine in the treatment of gout. Clin Ther 2014;36:1465–1479. - PubMed
-
- Vaidya K, Tucker B, Kurup R, Khandkar C, Pandzic E, Barraclough J, Machet J, Misra A, Kavurma M, Martinez G, Rye KA, Cochran BJ, Patel S. Colchicine inhibits neutrophil extracellular trap formation in patients with acute coronary syndrome after percutaneous coronary intervention. J Am Heart Assoc 2021;10:e018993. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
