

Pulsed field ablation selectively spares the oesophagus during pulmonary vein isolation for atrial fibrillation
- PMID: 33961027
- PMCID: PMC8427383
- DOI: 10.1093/europace/euab090
Pulsed field ablation selectively spares the oesophagus during pulmonary vein isolation for atrial fibrillation
Abstract
Aims: Extra-atrial injury can cause complications after catheter ablation for atrial fibrillation (AF). Pulsed field ablation (PFA) has generated preclinical data suggesting that it selectively targets the myocardium. We sought to characterize extra-atrial injuries after pulmonary vein isolation (PVI) between PFA and thermal ablation methods.
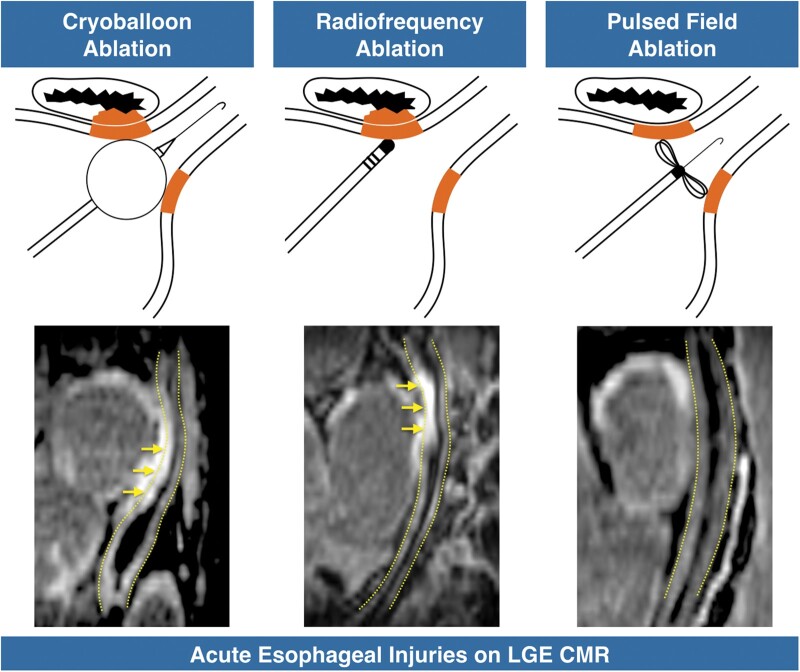
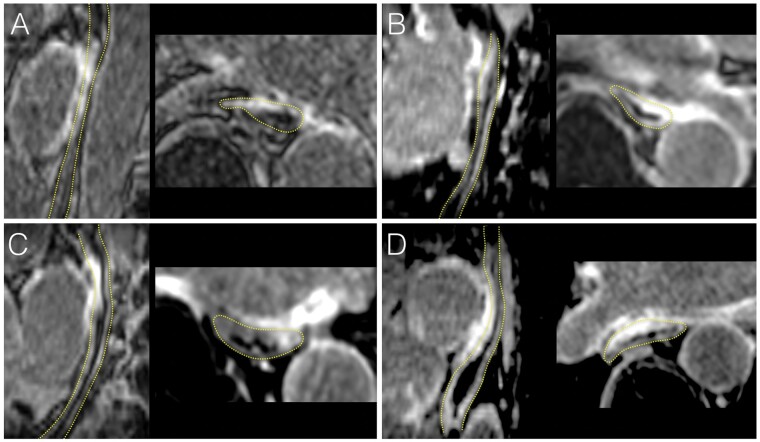
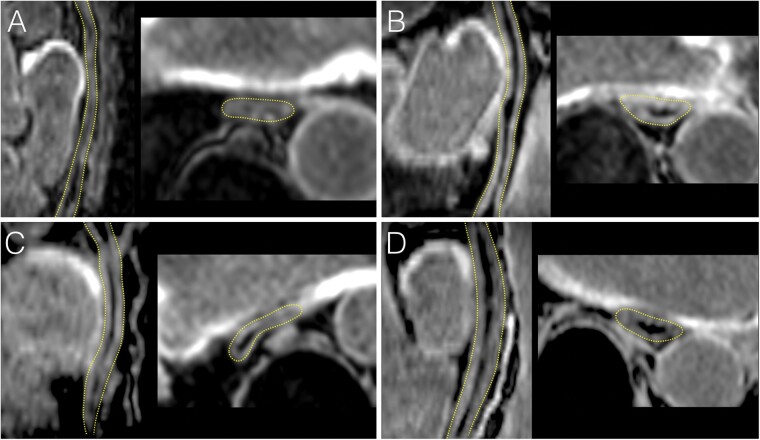
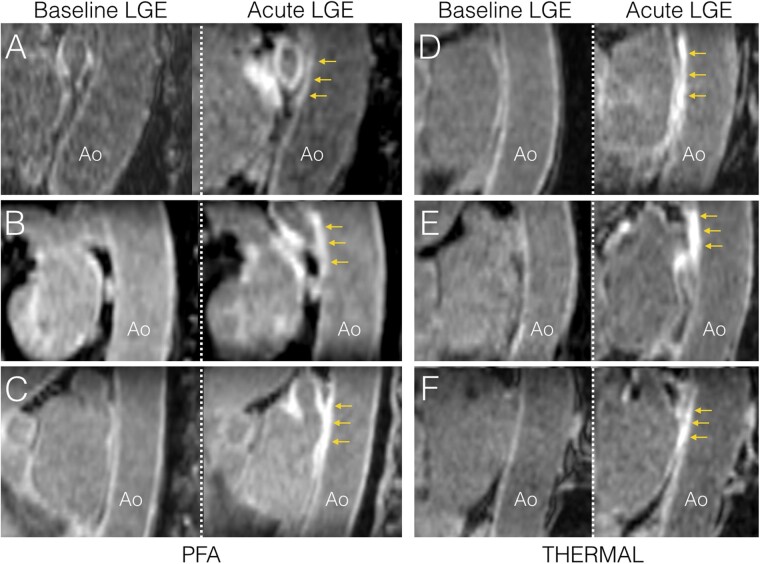
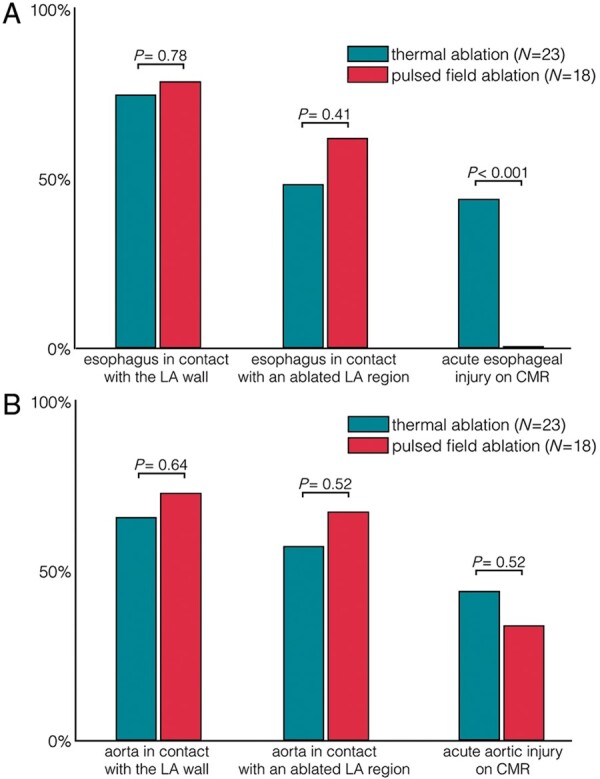
Methods and results: Cardiac magnetic resonance (CMR) imaging was performed before, acutely (<3 h) and 3 months post-ablation in 41 paroxysmal AF patients undergoing PVI with PFA (N = 18, Farapulse) or thermal methods (N = 23, 16 radiofrequency, 7 cryoballoon). Oesophageal and aortic injuries were assessed by using late gadolinium-enhanced (LGE) imaging. Phrenic nerve injuries were assessed from diaphragmatic motion on intra-procedural fluoroscopy. Baseline CMR showed no abnormality on the oesophagus or aorta. During ablation procedures, no patient showed phrenic palsy. Acutely, thermal methods induced high rates of oesophageal lesions (43%), all observed in patients showing direct contact between the oesophagus and the ablation sites. In contrast, oesophageal lesions were observed in no patient ablated with PFA (0%, P < 0.001 vs. thermal methods), despite similar rates of direct contact between the oesophagus and the ablation sites (P = 0.41). Acute lesions were detected on CMR on the descending aorta in 10/23 (43%) after thermal ablation, and in 6/18 (33%) after PFA (P = 0.52). CMR at 3 months showed a complete resolution of oesophageal and aortic LGE in all patients. No patient showed clinical complications.
Conclusion: PFA does not induce any signs of oesophageal injury on CMR after PVI. Due to its tissue selectivity, PFA may improve safety for catheter ablation of AF.
Keywords: Atrial fibrillation; Cardiac magnetic resonance; Catheter ablation; Oesophagus; Pulsed field ablation.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr. et al.; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2014;64:e1–76. - PubMed
-
- Wilber DJ, Pappone C, Neuzil P, De Paola A, Marchlinski F, Natale A. et al.; ThermoCool AF Trial Investigators. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA 2010;303:333–40. - PubMed
-
- Packer DL, Kowal RC, Wheelan KR, Irwin JM, Champagne J, Guerra PG. et al.; STOP AF Cryoablation Investigators. Cryoballoon ablation of pulmonary veins for paroxysmal atrial fibrillation: first results of the North American Arctic Front (STOP AF) pivotal trial. J Am Coll Cardiol 2013;61:1713–23. - PubMed
-
- Knopp H, Halm U, Lamberts R, Knigge I, Zachäus M, Sommer P. et al.Incidental and ablation-induced findings during upper gastrointestinal endoscopy in patients after ablation of atrial fibrillation: a retrospective study of 425 patients. Heart Rhythm 2014;11:574–8. - PubMed
-
- Sacher F, Monahan KH, Thomas SP, Davidson N, Adragao P, Sanders P. et al.Phrenic nerve injury after atrial fibrillation catheter ablation: characterization and outcome in a multicenter study. J Am Coll Cardiol 2006;47:2498–503. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
