

Comparison of Treatments for Cocaine Use Disorder Among Adults: A Systematic Review and Meta-analysis
- PMID: 33961037
- PMCID: PMC8105751
- DOI: 10.1001/jamanetworkopen.2021.8049
Comparison of Treatments for Cocaine Use Disorder Among Adults: A Systematic Review and Meta-analysis
Abstract
Importance: In the US and the United Kingdom, cocaine use is the second leading cause of illicit drug overdose death. Psychosocial treatments for cocaine use disorder are limited, and no pharmacotherapy is approved for use in the US or Europe.
Objective: To compare treatments for active cocaine use among adults.
Data sources: PubMed and the Cochrane Database of Systematic Reviews were searched for clinical trials published between December 31, 1995, and December 31, 2017.
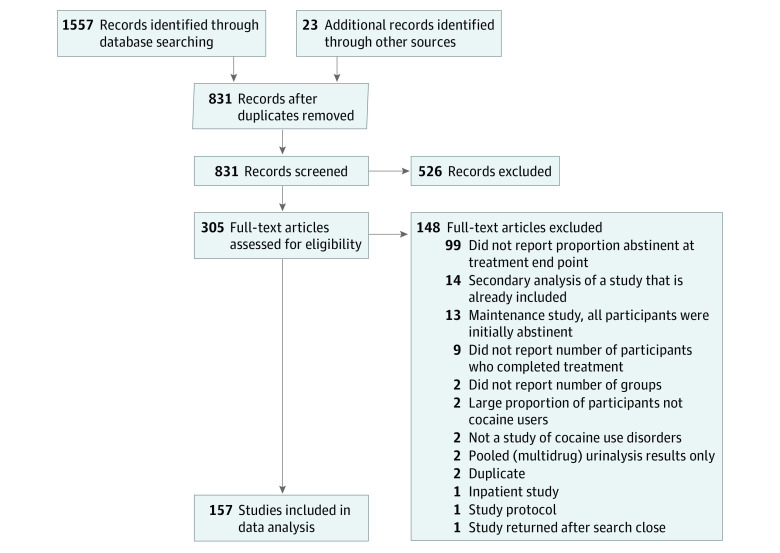
Study selection: This meta-analysis was registered on Covidence.org (study 8731) on December 31, 2015. Clinical trials were included if they (1) had the term cocaine in the article title; (2) were published between December 31, 1995, and December 31, 2017; (3) were written in English; (4) enrolled outpatients 18 years or older with active cocaine use at baseline; and (5) reported treatment group size, treatment duration, retention rates, and urinalysis results for the presence of cocaine metabolites. A study was excluded if (1) more than 25% of participants were not active cocaine users or more than 80% of participants had negative test results for the presence of cocaine metabolites at baseline and (2) it reported only pooled urinalysis results indicating the presence of multiple substances and did not report the specific proportion of positive test results for cocaine metabolites. Multiple reviewers reached criteria consensus. Of 831 records screened, 157 studies (18.9%) met selection criteria and were included in the analysis.
Data extraction and synthesis: This study followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guideline. Search results were imported from PubMed XML into Covidence.org then Microsoft Excel. Data extraction was completed in 2 iterations to ensure fidelity. Analyses included a multilevel random-effects model, a multilevel mixed-effects meta-regression model, and sensitivity analyses. Treatments were clustered into 11 categories (psychotherapy, contingency management programs, placebo, opioids, psychostimulants, anticonvulsants, dopamine agonists, antidepressants, antipsychotics, miscellaneous medications, and other therapies). Missing data were imputed using multiple imputation by chained equations. The significance threshold for all analyses was P = .05. Data were analyzed using the metafor and mice packages in R software, version 3.3.2 (R Foundation for Statistical Computing). Data were analyzed from January 1, 2018, to February 28, 2021.
Main outcomes and measures: The primary outcome was the intention-to-treat logarithm of the odds ratio (OR) of having a negative urinalysis result for the presence of cocaine metabolites at the end of each treatment period compared with baseline. The hypothesis, which was formulated after data collection, was that no treatment category would have a significant association with objective reductions in cocaine use.
Results: A total of 157 studies comprising 402 treatment groups and 15 842 participants were included. Excluding other therapies, the largest treatment groups across all studies were psychotherapy (mean [SD] number of participants, 40.04 [36.88]) and contingency management programs (mean [SD] number of participants, 37.51 [25.51]). Only contingency management programs were significantly associated with an increased likelihood of having a negative test result for the presence of cocaine (OR, 2.13; 95% CI, 1.62-2.80), and this association remained significant in all sensitivity analyses.
Conclusions and relevance: In this meta-analysis, contingency management programs were associated with reductions in cocaine use among adults. Research efforts and policies that align with this treatment modality may benefit those who actively use cocaine and attenuate societal burdens.
Conflict of interest statement
Similar articles
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Beyond the black stump: rapid reviews of health research issues affecting regional, rural and remote Australia.Med J Aust. 2020 Dec;213 Suppl 11:S3-S32.e1. doi: 10.5694/mja2.50881. Med J Aust. 2020. PMID: 33314144
-
Pharmacotherapy for Cocaine Use Disorder-a Systematic Review and Meta-analysis.J Gen Intern Med. 2019 Dec;34(12):2858-2873. doi: 10.1007/s11606-019-05074-8. Epub 2019 Jun 10. J Gen Intern Med. 2019. PMID: 31183685 Free PMC article.
-
Predictors of cocaine use disorder treatment outcomes: a systematic review.Syst Rev. 2024 May 8;13(1):124. doi: 10.1186/s13643-024-02550-z. Syst Rev. 2024. PMID: 38720357 Free PMC article.
-
Psychological interventions to improve self-management of type 1 and type 2 diabetes: a systematic review.Health Technol Assess. 2020 Jun;24(28):1-232. doi: 10.3310/hta24280. Health Technol Assess. 2020. PMID: 32568666 Free PMC article.
Cited by
-
Cocaine-Induced Locomotor Activation Differs Across Inbred Mouse Substrains.Front Psychiatry. 2022 May 6;13:800245. doi: 10.3389/fpsyt.2022.800245. eCollection 2022. Front Psychiatry. 2022. PMID: 35599758 Free PMC article.
-
Optimizing Contingency Management with Reinforcement Learning.medRxiv [Preprint]. 2024 Mar 29:2024.03.28.24305031. doi: 10.1101/2024.03.28.24305031. medRxiv. 2024. PMID: 38585900 Free PMC article. Preprint.
-
Getting Inside the Mind of Gay and Bisexual Men Who Have Sex with Men with Sexualized Drug Use - A Systematic Review.Int J Sex Health. 2023 Nov 29;35(4):573-595. doi: 10.1080/19317611.2023.2260372. eCollection 2023. Int J Sex Health. 2023. PMID: 38601804 Free PMC article.
-
Opposing Spatially Segregated Function of Endogenous GDNF-RET Signaling in Cocaine Addiction.Biomolecules. 2023 Apr 27;13(5):761. doi: 10.3390/biom13050761. Biomolecules. 2023. PMID: 37238631 Free PMC article.
-
Influence of cocaine use reduction on markers of immune function.J Neuroimmunol. 2024 Dec 15;397:578470. doi: 10.1016/j.jneuroim.2024.578470. Epub 2024 Oct 28. J Neuroimmunol. 2024. PMID: 39504756 Clinical Trial.
References
-
- Hedegaard H, Minino AM, Warner M. Drug overdose deaths in the United States, 1999-2018. NCHS Data Brief. 2020;(356):1-8. - PubMed
-
- European Monitoring Centre for Drugs and Drug Addiction . United Kingdom country drug report 2019. European Monitoring Centre for Drugs and Drug Addiction; 2019. Accessed April 4, 2020. https://www.emcdda.europa.eu/system/files/publications/11355/united-king...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
