

Restrictive fluid management versus usual care in acute kidney injury (REVERSE-AKI): a pilot randomized controlled feasibility trial
- PMID: 33961058
- PMCID: PMC8195764
- DOI: 10.1007/s00134-021-06401-6
Restrictive fluid management versus usual care in acute kidney injury (REVERSE-AKI): a pilot randomized controlled feasibility trial
Abstract
Purpose: We compared a restrictive fluid management strategy to usual care among critically ill patients with acute kidney injury (AKI) who had received initial fluid resuscitation.
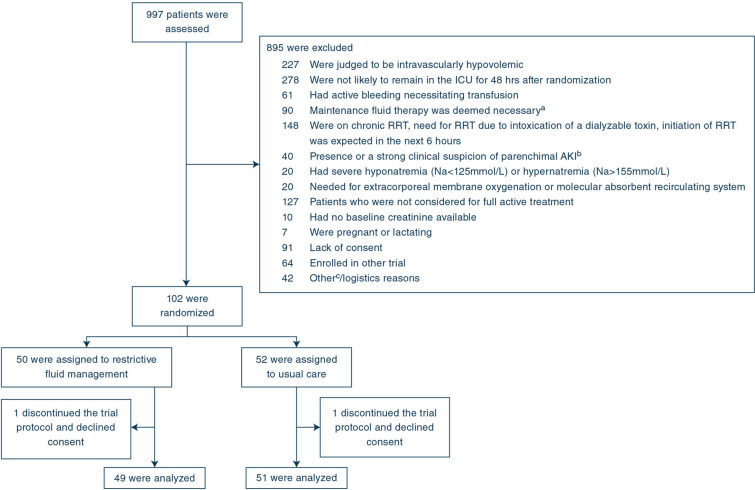
Methods: This multicenter feasibility trial randomized 100 AKI patients 1:1 in seven ICUs in Europe and Australia. Restrictive fluid management included targeting negative or neutral daily fluid balance by minimizing fluid input and/or enhancing urine output with diuretics administered at the discretion of the clinician. Fluid boluses were administered as clinically indicated. The primary endpoint was cumulative fluid balance 72 h from randomization.
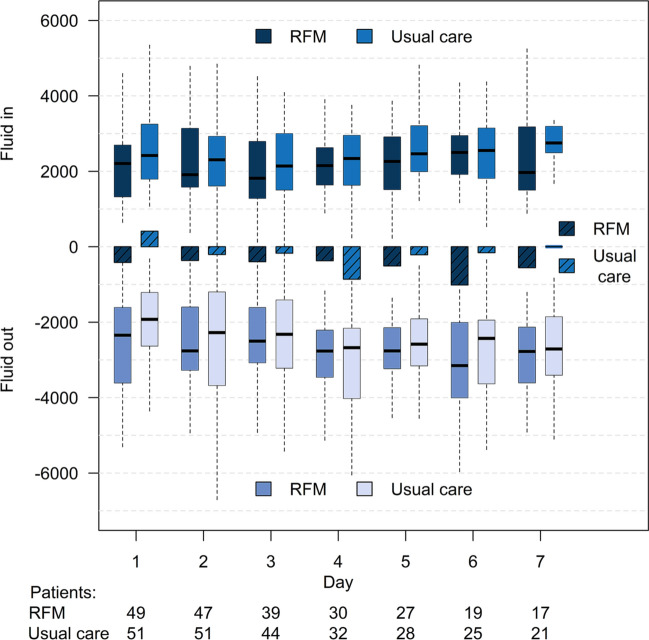
Results: Mean (SD) cumulative fluid balance at 72 h from randomization was - 1080 mL (2003 mL) in the restrictive fluid management arm and 61 mL (3131 mL) in the usual care arm, mean difference (95% CI) - 1148 mL (- 2200 to - 96) mL, P = 0.033. Median [IQR] duration of AKI was 2 [1-3] and 3 [2-7] days, respectively (median difference - 1.0 [- 3.0 to 0.0], P = 0.071). Altogether, 6 out of 46 (13%) patients in the restrictive fluid management arm and 15 out of 50 (30%) in the usual care arm received renal replacement therapy (RR 0.42; 95% CI 0.16-0.91), P = 0.043. Cumulative fluid balance at 24 h and 7 days was lower in the restrictive fluid management arm. The dose of diuretics was not different between the groups. Adverse events occurred more frequently in the usual care arm.
Conclusions: In critically ill patients with AKI, a restrictive fluid management regimen resulted in lower cumulative fluid balance and less adverse events compared to usual care. Larger trials of this intervention are justified.
Keywords: Acute kidney injury; Critically ill; Fluid balance; Restrictive fluid management.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- KDIGO (2012) KDIGO clinical practice guideline for acute kidney injury. Kidney Inter Suppl 1–138
-
- Meersch M, Schmidt C, Hoffmeier A, Van Aken H, Wempe C, Gerss J, et al. Prevention of cardiac surgery-associated AKI by implementing the KDIGO guidelines in high risk patients identified by biomarkers: the PrevAKI randomized controlled trial. Intensive Care Med. 2017;43:1551–1561. doi: 10.1007/s00134-016-4670-3. - DOI - PMC - PubMed
-
- Pickkers P, Mehta RL, Murray PT, Joannidis M, Molitoris BA, Kellum JA, et al. Effect of human recombinant alkaline phosphatase on 7-day creatinine clearance in patients with sepsis-associated acute kidney injury: a randomized clinical trial. JAMA. 2018;320:1998–2009. doi: 10.1001/jama.2018.14283. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
