

Tissue-based SARS-CoV-2 detection in fatal COVID-19 infections: Sustained direct viral-induced damage is not necessary to drive disease progression
- PMID: 33961839
- PMCID: PMC8095022
- DOI: 10.1016/j.humpath.2021.04.012
Tissue-based SARS-CoV-2 detection in fatal COVID-19 infections: Sustained direct viral-induced damage is not necessary to drive disease progression
Abstract
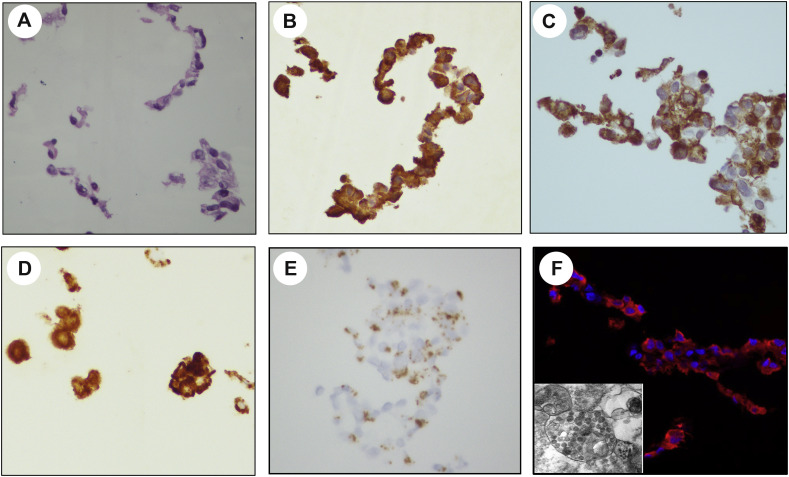
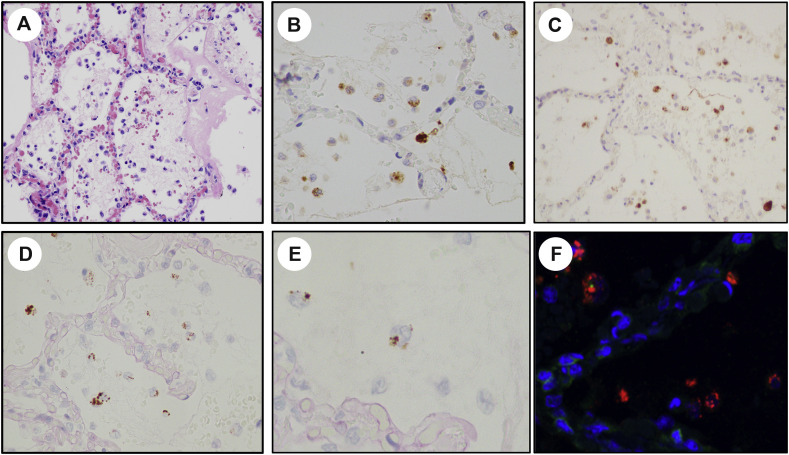
Coronavirus disease 2019 (COVID-19) is an ongoing pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Although viral infection is known to trigger inflammatory processes contributing to tissue injury and organ failure, it is unclear whether direct viral damage is needed to sustain cellular injury. An understanding of pathogenic mechanisms has been handicapped by the absence of optimized methods to visualize the presence and distribution of SARS-CoV-2 in damaged tissues. We first developed a positive control cell line (Vero E6) to validate SARS-CoV-2 detection assays. We then evaluated multiple organs (lungs, kidneys, heart, liver, brain, intestines, lymph nodes, and spleen) from fourteen COVID-19 autopsy cases using immunohistochemistry (IHC) for the spike and the nucleoprotein proteins, and RNA in situ hybridization (RNA ISH) for the spike protein mRNA. Tissue detection assays were compared with quantitative polymerase chain reaction (qPCR)-based detection. SARS-CoV-2 was histologically detected in the Vero E6 positive cell line control, 1 of 14 (7%) lungs, and none (0%) of the other 59 organs. There was perfect concordance between the IHC and RNA ISH results. qPCR confirmed high viral load in the SARS-CoV-2 ISH-positive lung tissue, and absent or low viral load in all ISH-negative tissues. In patients who die of COVID-19-related organ failure, SARS-CoV-2 is largely not detectable using tissue-based assays. Even in lungs showing widespread injury, SARS-CoV-2 viral RNA or proteins were detected in only a small minority of cases. This observation supports the concept that viral infection is primarily a trigger for multiple-organ pathogenic proinflammatory responses. Direct viral tissue damage is a transient phenomenon that is generally not sustained throughout disease progression.
Keywords: COVID-19; Coronavirus; Diffuse alveolar damage; Nucleoprotein; RNA in situ hybridization; SARS-CoV-2; Spike protein.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
COVID-19: Multiorgan Dissemination of SARS-CoV-2 Is Driven by Pulmonary Factors.Viruses. 2021 Dec 26;14(1):39. doi: 10.3390/v14010039. Viruses. 2021. PMID: 35062243 Free PMC article.
-
Comparison of RNA In Situ Hybridization and Immunohistochemistry Techniques for the Detection and Localization of SARS-CoV-2 in Human Tissues.Am J Surg Pathol. 2021 Jan;45(1):14-24. doi: 10.1097/PAS.0000000000001563. Am J Surg Pathol. 2021. PMID: 32826529
-
Evidence of Severe Acute Respiratory Syndrome Coronavirus 2 Replication and Tropism in the Lungs, Airways, and Vascular Endothelium of Patients With Fatal Coronavirus Disease 2019: An Autopsy Case Series.J Infect Dis. 2021 Mar 3;223(5):752-764. doi: 10.1093/infdis/jiab039. J Infect Dis. 2021. PMID: 33502471 Free PMC article.
-
Pathological findings in organs and tissues of patients with COVID-19: A systematic review.PLoS One. 2021 Apr 28;16(4):e0250708. doi: 10.1371/journal.pone.0250708. eCollection 2021. PLoS One. 2021. PMID: 33909679 Free PMC article.
-
Detection of SARS-CoV-2 in Neonatal Autopsy Tissues and Placenta.Emerg Infect Dis. 2022 Mar;28(3):510-517. doi: 10.3201/eid2803.211735. Epub 2022 Feb 9. Emerg Infect Dis. 2022. PMID: 35138244 Free PMC article. Review.
Cited by
-
Identification of Clinical Response Predictors of Tocilizumab Treatment in Patients with Severe COVID-19 Based on Single-Center Experience.J Clin Med. 2023 Mar 22;12(6):2429. doi: 10.3390/jcm12062429. J Clin Med. 2023. PMID: 36983429 Free PMC article.
-
COVID-19: Multiorgan Dissemination of SARS-CoV-2 Is Driven by Pulmonary Factors.Viruses. 2021 Dec 26;14(1):39. doi: 10.3390/v14010039. Viruses. 2021. PMID: 35062243 Free PMC article.
-
SARS-CoV-2-Infection (COVID-19): Clinical Course, Viral Acute Respiratory Distress Syndrome (ARDS) and Cause(s) of Death.Med Sci (Basel). 2022 Oct 10;10(4):58. doi: 10.3390/medsci10040058. Med Sci (Basel). 2022. PMID: 36278528 Free PMC article. Review.
-
Olfactory Bulb and Amygdala Gene Expression Changes in Subjects Dying with COVID-19.medRxiv [Preprint]. 2021 Sep 15:2021.09.12.21263291. doi: 10.1101/2021.09.12.21263291. medRxiv. 2021. PMID: 34545375 Free PMC article. Preprint.
-
SARS-Cov-2 infection and neuropathological findings: a report of 18 cases and review of the literature.Acta Neuropathol Commun. 2023 May 10;11(1):78. doi: 10.1186/s40478-023-01566-1. Acta Neuropathol Commun. 2023. PMID: 37165453 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
