

Diagnostic pitfalls: intramyocardial lymphoma metastasis mimics acute coronary syndrome in a diffuse large B cell lymphoma patient-case report
- PMID: 33962562
- PMCID: PMC8103629
- DOI: 10.1186/s12245-021-00352-x
Diagnostic pitfalls: intramyocardial lymphoma metastasis mimics acute coronary syndrome in a diffuse large B cell lymphoma patient-case report
Abstract
Background: Cardiac tumors are very uncommon compared to other cardiac diseases. Their clinical symptoms can vary from absent to non-specific. The most common symptoms are arrhythmias, blood flow obstruction due to valvular dysfunction, shortness of breath, systemic embolization, and accumulation of pericardial fluid. Hereby, we describe a very rare case of a diffuse large B cell lymphoma patient who presented with the symptoms and signs of acute coronary syndrome (ACS) but the patient's complaints were caused by his intramyocardial lymphoma metastasis.
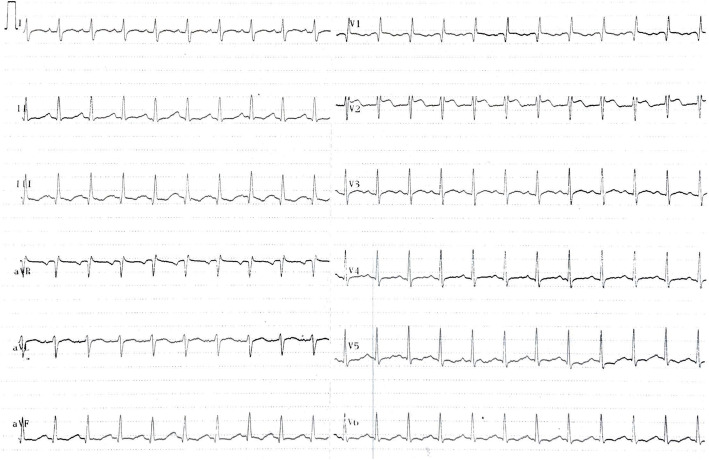
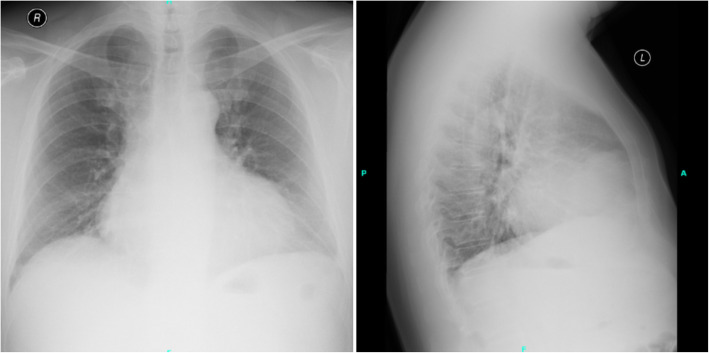
Case presentation: Forty-eight-year-old diffuse large B cell lymphoma patient was admitted to our emergency department with chest pain, effort dyspnea, and fever. The patient had normal blood pressure, blood oxygen saturation, sinus tachycardia, fever, crackles over the left lower lobe, novum incomplete right bundle branch block with Q waves and minor ST alterations, elevated C-reactive protein, high-sensitivity troponin-T, and d-dimer levels. Chest X-ray revealed consolidation on the left side and enlarged heart. Bed side transthoracic echocardiography showed inferior akinesis with pericardial fluid. Coronary angiography showed no occlusion or significant stenosis. Chest computed tomography demonstrated the progression of his lymphoma in the myocardium. He was admitted to the Department of Hematology for immediate chemotherapy and he reached complete metabolic remission, followed by allogeneic hematopoietic stem cell transplantation. Unfortunately, about 9 months later, he developed bone marrow deficiency consequently severe sepsis, septic shock, and multiple organ failure what he did not survive.
Conclusions: Our case demonstrates a very rare manifestation of a heart metastasis. ACS is an unusual symptom of cardiac tumors. But our patient's intramyocardial lymphoma in the right atrium and ventricle externally compressed the right coronary artery and damaged the heart tissue, causing the patient's symptoms which imitated ACS. Fortunately, the quick diagnostics and immediate aggressive chemotherapy provided the patient's remission and suitability to further treatment.
Keywords: Acute coronary syndrome; Cardiac metastasis; Coronary artery; Differential diagnosis; Diffuse large B cell lymphoma.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Centofanti P, Di Rosa E, Deorsola L, Actis Dato GM, Patanè F, La Torre M, et al. Primary cardiac tumors: Early and late results of surgical treatment in 91 patients. Ann Thorac Surg. 1999;68:1236–41. 10.1016/S0003-4975(99)00700-6. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
