

Double kissing inflation outside the stent secures the patency of small side branch without rewiring
- PMID: 33962571
- PMCID: PMC8106182
- DOI: 10.1186/s12872-021-02028-z
Double kissing inflation outside the stent secures the patency of small side branch without rewiring
Abstract
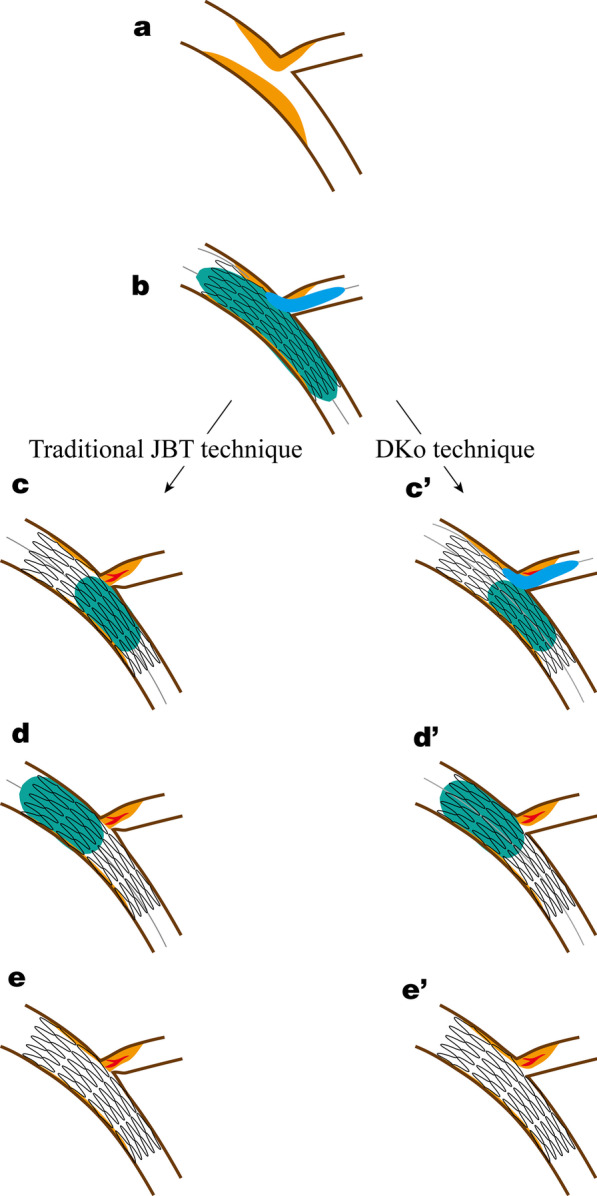
Background: The jailed balloon technique is widely used for coronary bifurcation lesions, but a residual risk of SB occlusion remains, necessitating SB rewiring and further interventions, including balloon inflation or stenting, which may result in failure and SB loss. This study introduced a novel modified technique of small side branch (SB) protection, namely, double kissing inflation outside the stent (DKo) technique, for coronary bifurcations without the need for SB rewiring.
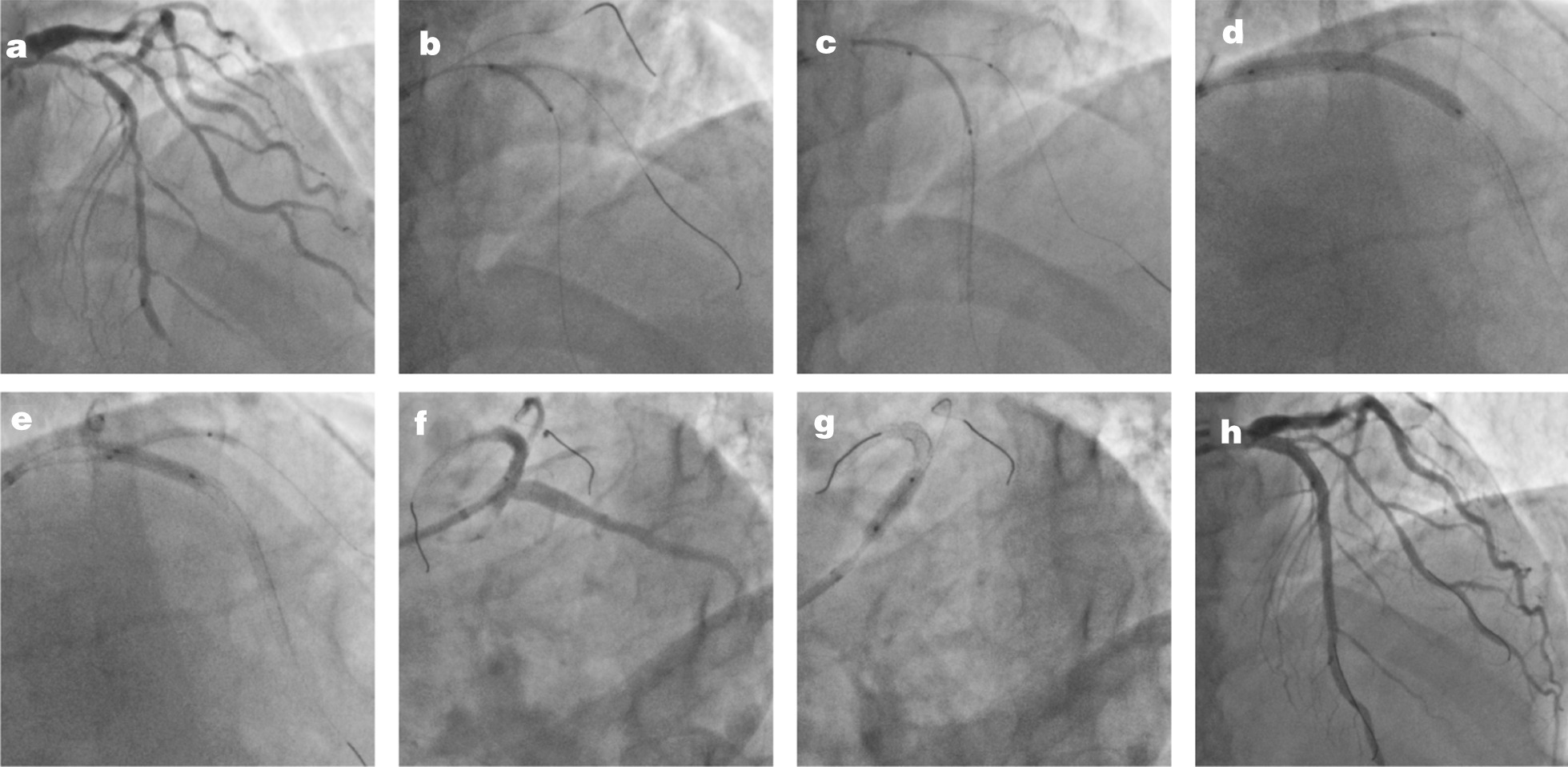
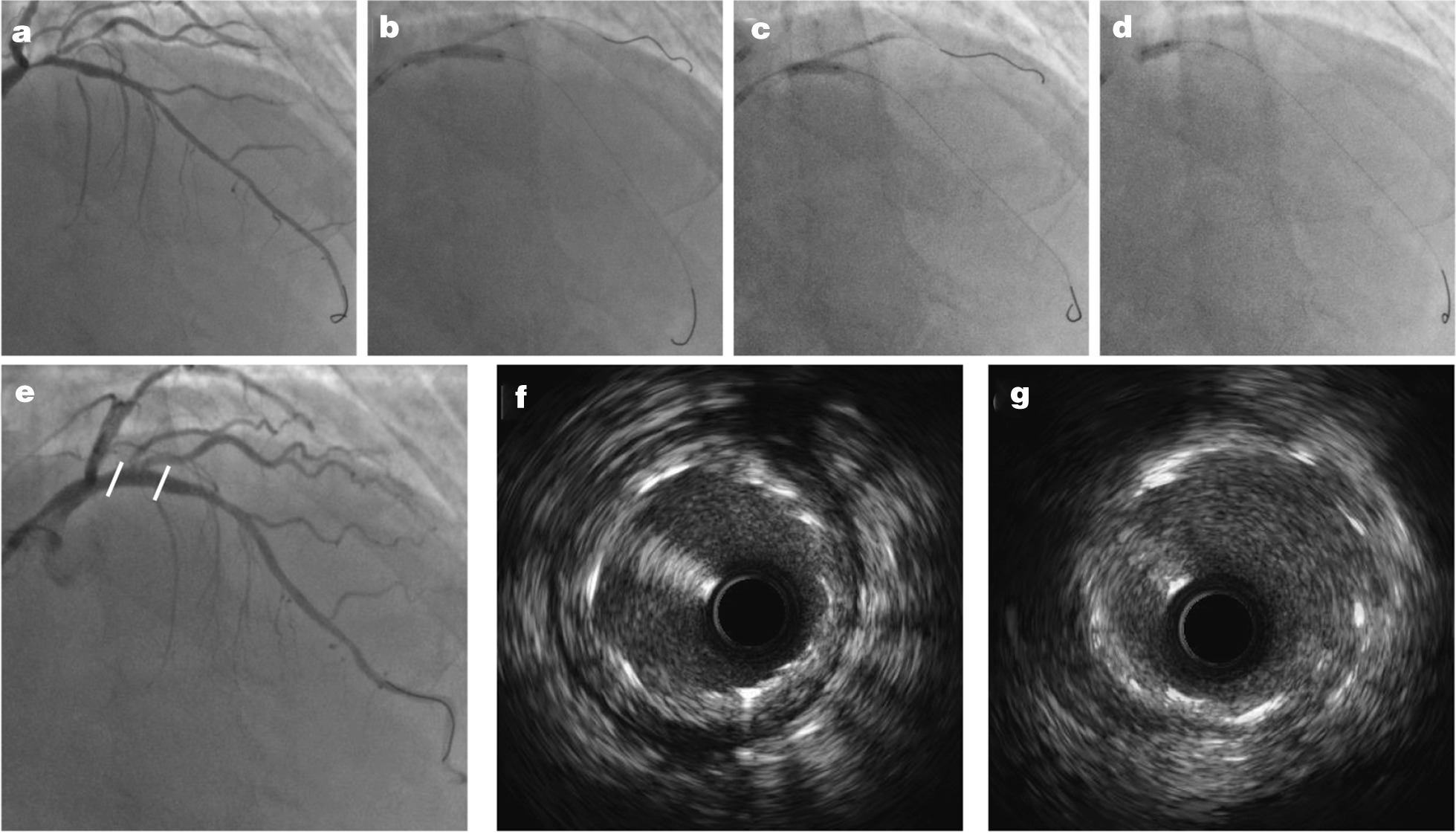
Methods: We performed the DKo technique in consecutive patients in our center from 1/2019 to 12/2019. The procedure was as follows. We inserted a guide wire into both branches followed by proper preparation. The SB balloon was simultaneously inflated with main vessel (MV) stenting. The SB balloon remained in situ until it was kissing inflated with postdilation of the bifurcation core, which is different from traditional strategies. The proximal optimization technique was performed with a short noncompliant balloon strictly not exceeding the bifurcation. Rates of SB loss and in-hospital outcomes were evaluated.
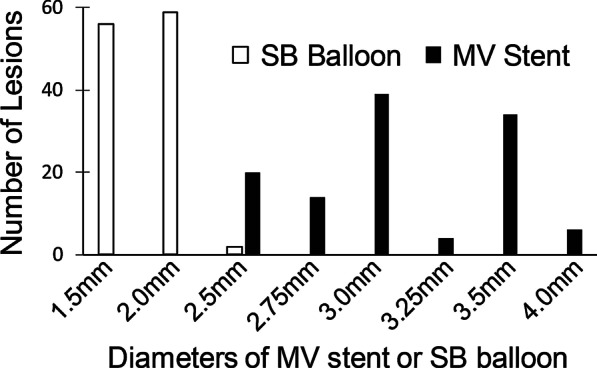
Results: The technique was successfully performed in all 117 enrolled patients without any rewiring or SB loss. The mean lesion lengths of the MV and SB were 38.3 ± 19.9 mm and 11.7 ± 7.1 mm, respectively. On average, 1.5 ± 0.6 stents were used per patient, while the mean pressure of the SB balloon was 7.4 ± 3.1 atm. DKo achieved excellent procedural success in the proximal and distal MVs: increased minimal lumen diameter (0.64 ± 0.58 mm to 3.05 ± 0.38 mm, p < 0.001; 0.57 ± 0.63 mm to 2.67 ± 0.35 mm, p < 0.001) and low residual stenosis (11.4 ± 3.4%; 7.2 ± 4.6%). DKo secured the patency of the SB without any rewiring and improved the SB stenosis with minimal lumen diameter (0.59 ± 0.48 mm to 1.20 ± 0.42 mm, p < 0.001) and stenosis (71.9 ± 19.4% to 42.2 ± 14.0%, p < 0.001). No MACE was noted in the hospital.
Conclusions: DKo for bifurcation lesions was shown to be acceptable with high procedural success and excellent SB protection.
Keywords: Coronary bifurcation lesion; Kissing balloon inflation; Percutaneous coronary intervention; Side branch protection.
Conflict of interest statement
All authors declare no competing financial interests.
Figures
References
-
- Di Gioia G, Sonck J, Ferenc M, Chen SL, Colaiori I, Gallinoro E, et al. Clinical outcomes following coronary bifurcation PCI techniques: a systematic review and network meta-analysis comprising 5,711 patients. JACC Cardiovasc Interv. 2020;13(12):1432–1444. doi: 10.1016/j.jcin.2020.03.054. - DOI - PubMed
-
- Crimi G, Mandurino-Mirizzi A, Gritti V, Scotti V, Strozzi C, de Silvestri A, et al. Percutaneous coronary intervention techniques for bifurcation disease: network meta-analysis reveals superiority of double-kissing crush. Can J Cardiol. 2020;36(6):906–914. doi: 10.1016/j.cjca.2019.09.002. - DOI - PubMed
-
- Behan MW, Holm NR, de Belder AJ, Cockburn J, Erglis A, Curzen NP, et al. Coronary bifurcation lesions treated with simple or complex stenting: 5-year survival from patient-level pooled analysis of the Nordic Bifurcation Study and the British Bifurcation Coronary Study. Eur Heart J. 2016;37(24):1923–1928. doi: 10.1093/eurheartj/ehw170. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
