

Electromyographic features and efficacy of orofacial myofunctional treatment for skeletal anterior open bite in adolescents: an exploratory study
- PMID: 33962610
- PMCID: PMC8103572
- DOI: 10.1186/s12903-021-01605-0
Electromyographic features and efficacy of orofacial myofunctional treatment for skeletal anterior open bite in adolescents: an exploratory study
Abstract
Background: Due to the multifactorial aetiology and unpredictable long-term stability, skeletal anterior open bite (SAOB) is one of the most intractable conditions for orthodontists. The abnormal orofacial myofunctional status (OMS) may be a major risk factor contributing to the development and relapse of SAOB. This study is aimed at evaluating the OMS and the efficacy of orofacial myofunctional therapy (OMT) alone for SAOB subjects.
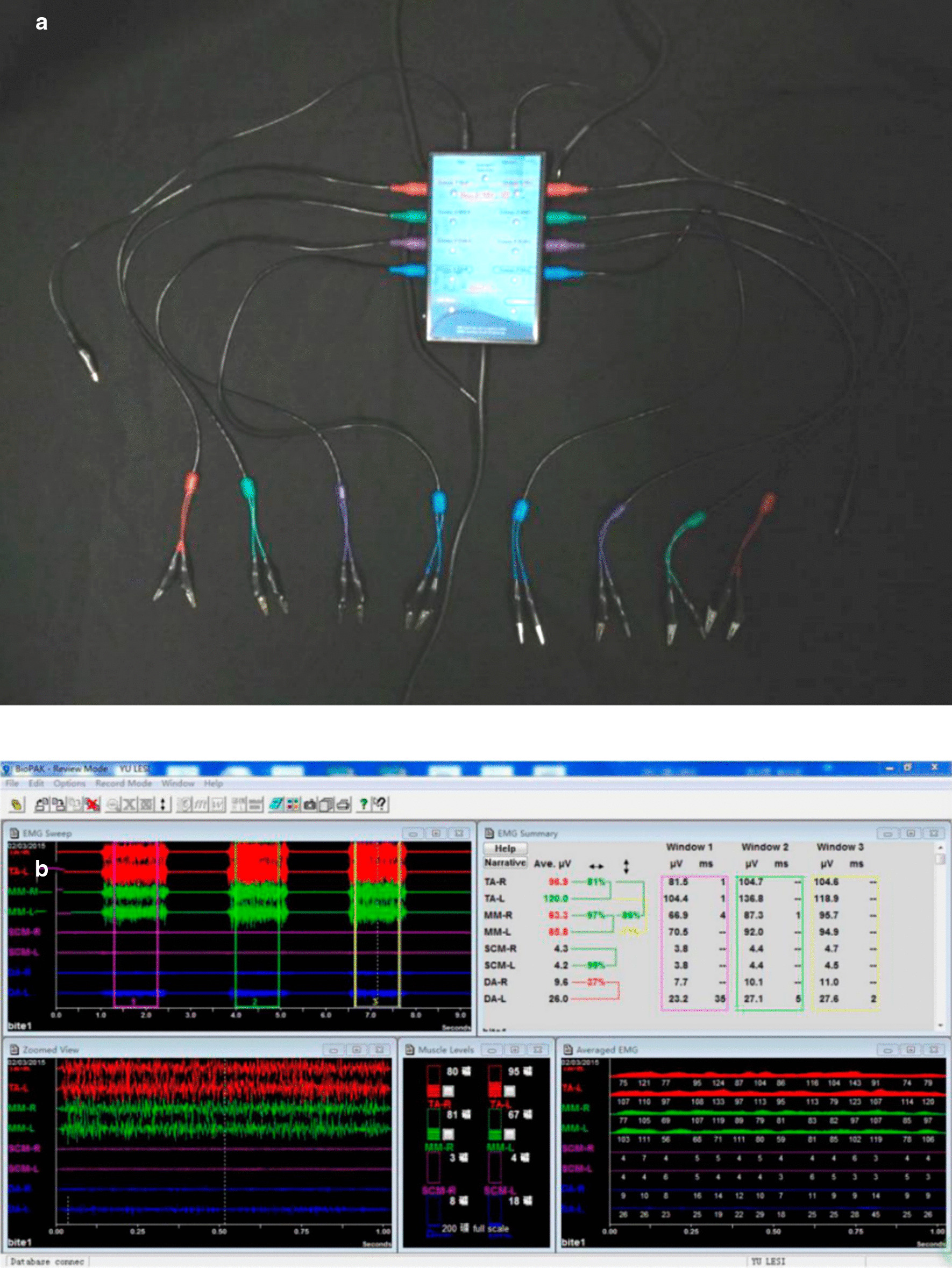
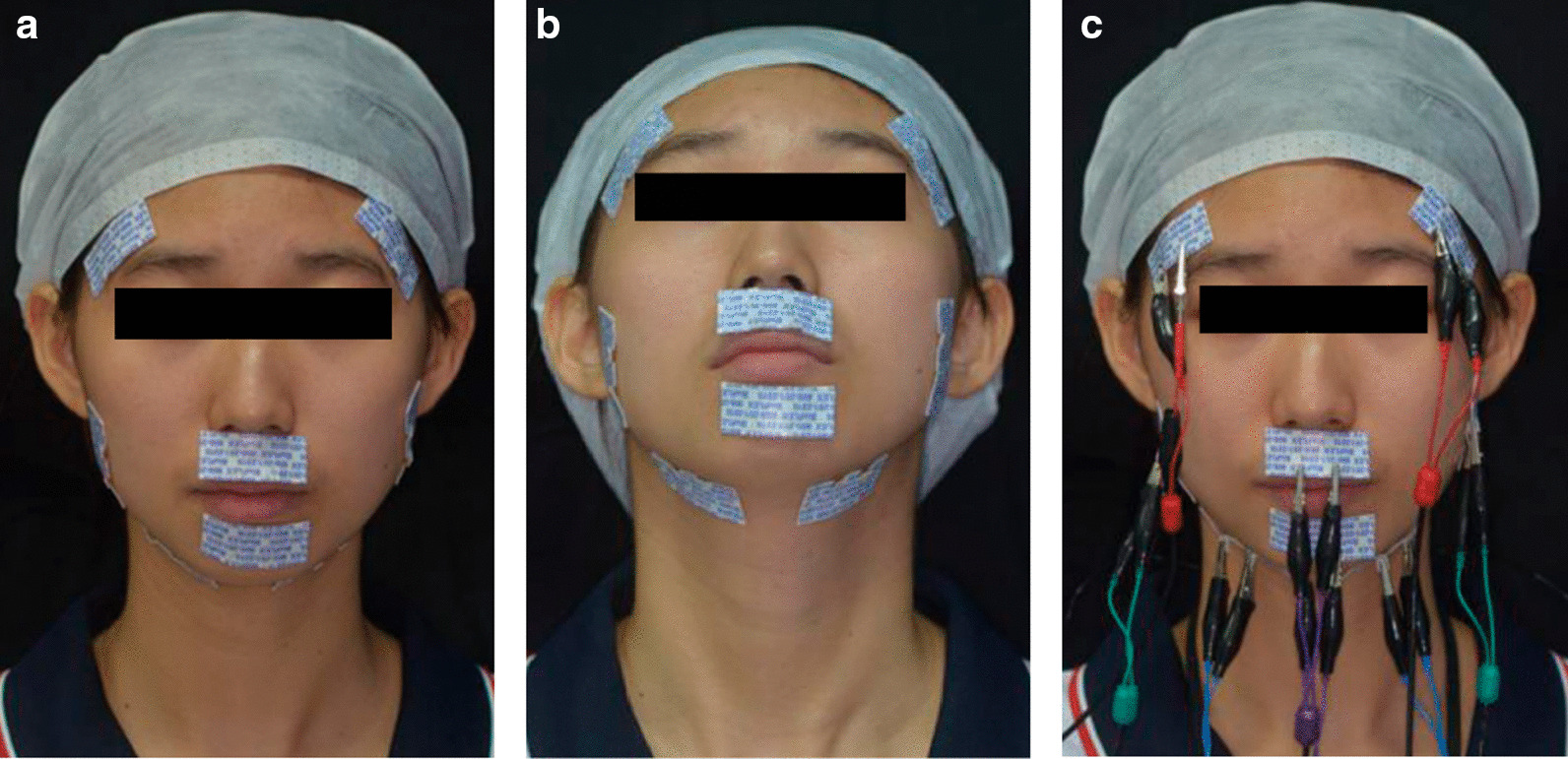
Methods: Eighteen adolescents with SAOB (4 males, 14 females; age: 12-18 years) and eighteen adolescents with normal occlusion (2 males, 16 females; age: 12-18 years) were selected. The electromyographic activity (EMGA) associated with mastication and closed mouth state was measured. Lateral cephalography was used to evaluate craniofacial morphology. Wilcoxon signed rank tests and t-tests were performed to evaluate myofunctional and morphological differences. Pearson or Spearman correlation analysis was used to investigate the correlations between EMGA and morphological characteristics. SAOB subjects were given OMT for 3 months, and the EMGA was compared between before and after OMT.
Results: During rest, anterior temporalis activity (TAA) and mentalis muscle activity (MEA) increased in SAOB subjects, but TAA and masseter muscle activity (MMA) decreased in the intercuspal position (ICP); and upper orbicularis activity (UOA) and MEA significantly increased during lip sealing and swallowing (P < 0.05). Morphological evaluation revealed increases in the FMA, GoGn-SN, ANS-Me, N-Me, L1-MP, U6-PP, and L6-MP and decreases in the angle of the axis of the upper and lower central incisors and OB in SAOB subjects (P < 0.05). TAA, MMA and anterior digastric activity (DAA) in the ICP were negatively correlated with vertical height and positively correlated to incisor protrusion. MEA was positively correlated with vertical height and negatively correlated with incisor protrusion; and the UOA showed a similar correlation in ICP, during sealing lip and swallowing. After SAOB subjects received OMT, MEA during rest and TAA, MMA and DAA in the ICP increased, while UOA and MEA decreased (P < 0.05).
Conclusion: SAOB subjects showed abnormal OMS features including aberrant swallowing patterns and weak masticatory muscles, which were interrelated with the craniofacial dysmorphology features including a greater anterior facial height and incisor protrusion. Furthermore, OMT contributes to OMS harmonization, indicating its therapeutic prospect in SAOB.
Keywords: Orofacial myofunctional status; Orofacial myofunctional therapy; Skeletal anterior open bite.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
The effect of orofacial myofunctional treatment in children with anterior open bite and tongue dysfunction: a pilot study.Eur J Orthod. 2016 Jun;38(3):227-34. doi: 10.1093/ejo/cjv044. Epub 2015 Jul 1. Eur J Orthod. 2016. PMID: 26136435 Free PMC article. Clinical Trial.
-
Relapse of anterior open bites treated with orthodontic appliances with and without orofacial myofunctional therapy.Am J Orthod Dentofacial Orthop. 2010 May;137(5):605-14. doi: 10.1016/j.ajodo.2008.07.016. Am J Orthod Dentofacial Orthop. 2010. PMID: 20451779
-
Effects of orofacial myofunctional therapy on masticatory function in individuals submitted to orthognathic surgery: a randomized trial.J Appl Oral Sci. 2018 Feb 1;26:e20170164. doi: 10.1590/1678-7757-2017-0164. J Appl Oral Sci. 2018. PMID: 29412368 Free PMC article. Clinical Trial.
-
Effect of orthodontic management and orofacial muscle training protocols on the correction of myofunctional and myoskeletal problems in developing dentition. A systematic review and meta-analysis.Orthod Craniofac Res. 2018 Nov;21(4):202-215. doi: 10.1111/ocr.12240. Epub 2018 Aug 27. Orthod Craniofac Res. 2018. PMID: 30152171
-
Effectiveness of orofacial myofunctional therapy in improving orofacial function and oral habits: a scoping review.Can J Dent Hyg. 2025 Feb 1;59(1):59-72. eCollection 2025 Feb. Can J Dent Hyg. 2025. PMID: 40166722 Free PMC article.
Cited by
-
Impact of initial lip competence on the outcome of class II functional appliances therapy.Clin Oral Investig. 2024 Jan 30;28(2):126. doi: 10.1007/s00784-024-05511-x. Clin Oral Investig. 2024. PMID: 38286891 Free PMC article.
-
Craniosynostosis: orofacial and oral health perspectives with masticatory insights.BMC Oral Health. 2024 Jul 8;24(1):767. doi: 10.1186/s12903-024-04540-y. BMC Oral Health. 2024. PMID: 38978035 Free PMC article.
-
Strategic treatment planning for anterior open bite: A comprehensive approach.J Dent Sci. 2024 Jul;19(3):1328-1337. doi: 10.1016/j.jds.2024.04.001. Epub 2024 Apr 16. J Dent Sci. 2024. PMID: 39035309 Free PMC article. Review.
-
Tongue Behavior in Anterior Open Bite-A Narrative Review.Diagnostics (Basel). 2025 Mar 14;15(6):724. doi: 10.3390/diagnostics15060724. Diagnostics (Basel). 2025. PMID: 40150067 Free PMC article. Review.
-
Effect of malocclusion on jaw motor function and chewing in children: a systematic review.Clin Oral Investig. 2022 Mar;26(3):2335-2351. doi: 10.1007/s00784-021-04356-y. Epub 2022 Jan 5. Clin Oral Investig. 2022. PMID: 34985577 Free PMC article.
References
-
- Taibah SM, Feteih RM. Cephalometric features of anterior open bite. World J Orthod. 2007;8(2):145–152. - PubMed
-
- Perillo L, Isola G, Esercizio D, Iovane M, Triolo G, Matarese G. Differences in craniofacial characteristics in Southern Italian children from Naples: a retrospective study by cephalometric analysis. Eur J Paediatr Dent. 2013;14(3):195–198. - PubMed
-
- Perillo L, Padricelli G, Isola G, Femiano F, Chiodini P, Matarese G. Class II malocclusion division 1: a new classification method by cephalometric analysis. Eur J Paediatr Dent. 2012;13(3):192–196. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
