

Long-term structural and symptomatic effects of intra-articular sprifermin in patients with knee osteoarthritis: 5-year results from the FORWARD study
- PMID: 33962962
- PMCID: PMC8292562
- DOI: 10.1136/annrheumdis-2020-219181
Long-term structural and symptomatic effects of intra-articular sprifermin in patients with knee osteoarthritis: 5-year results from the FORWARD study
Abstract
Objective: The FORWARD (FGF-18 Osteoarthritis Randomized Trial with Administration of Repeated Doses) trial assessed efficacy and safety of the potential disease-modifying osteoarthritis drug (DMOAD) sprifermin in patients with knee osteoarthritis. Here, we report 5-year efficacy and safety results.
Methods: Patients were randomised to intra-articular sprifermin 100 µg or 30 µg every 6 months (q6mo) or 12 months, or placebo, for 18 months. The primary analysis was at year 2, with follow-up at years 3, 4 and 5. Additional post hoc exploratory analyses were conducted in patients with baseline minimum radiographic joint space width 1.5-3.5 mm and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain 40-90, a subgroup at risk (SAR) of progression.
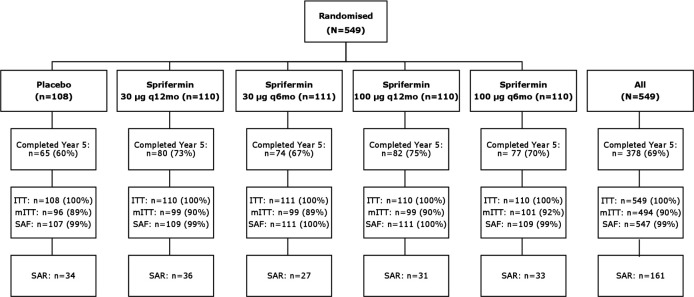
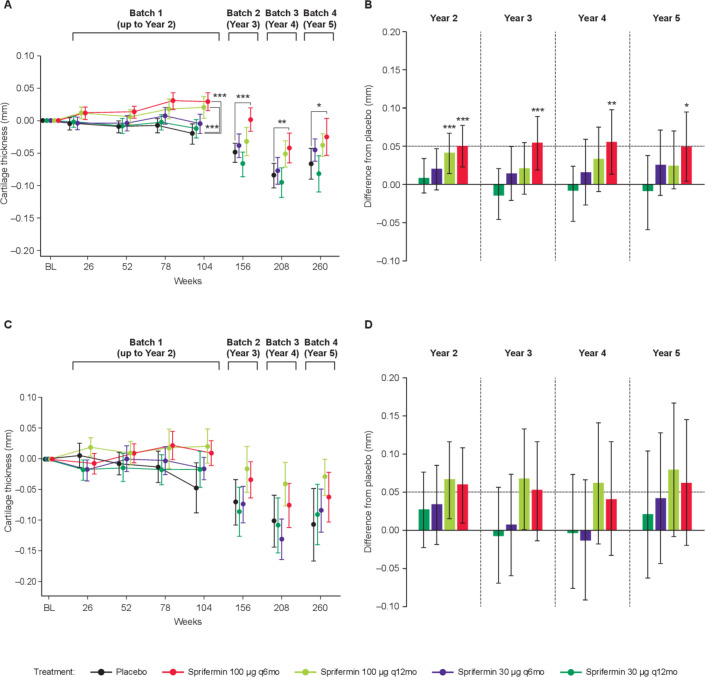
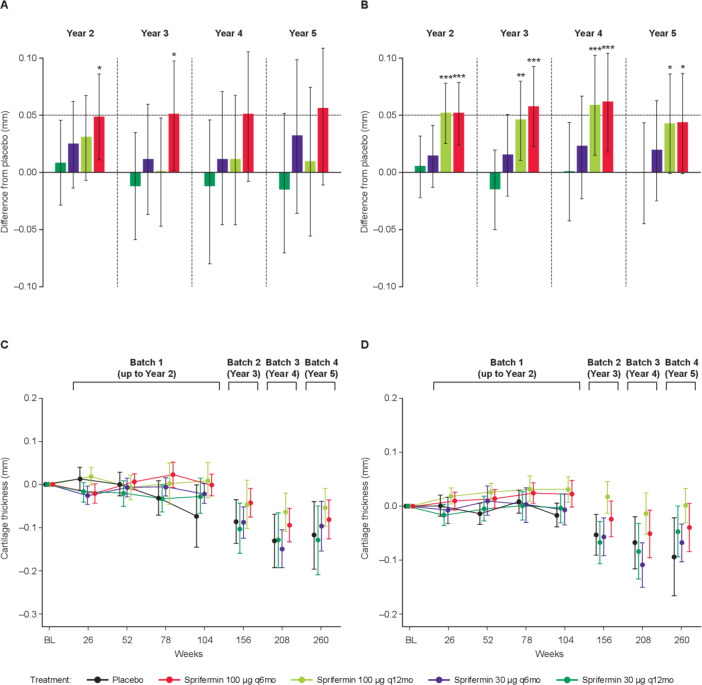
Results: 378 (69%) patients completed the 5-year follow-up. A significant dose-response in total femorotibial joint cartilage thickness with sprifermin (trend test, p<0.001) and a 0.05 mm mean difference with sprifermin 100 µg q6mo versus placebo (95% CI 0.00 to 0.10; p=0.015) were sustained to year 5. WOMAC pain scores improved ~50% from baseline in all groups. No patient in the 100 µg q6mo group had replacement of the treated knee. 96%-98% of patients receiving sprifermin and 98% placebo reported adverse events, most were mild or moderate and deemed unrelated to treatment. Adverse event-related study withdrawals were <10%. Differentiation in WOMAC pain between sprifermin 100 µg q6mo and placebo in the SAR (n=161) at year 3 was maintained to year 5 (-10.08; 95% CI -25.68 to 5.53).
Conclusion: In the longest DMOAD trial reported to date, sprifermin maintained long-term structural modification of articular cartilage over 3.5 years post-treatment. Potential translation to clinical benefit was observed in the SAR.
Trial registration number: NCT01919164.
Keywords: biological therapy; knee; magnetic resonance imaging; osteoarthritis; therapeutics.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: FE is an employee and co-owner of Chondrometrics GmbH and reported receiving grants and consulting fees from Merck KGaA, Darmstadt, Germany, Samumed LLC, AbbVie, Bioclinica, Orthotrophix, Kolon TissueGene, Servier, Roche, Galapagos, Novartis, ICM and Healthlink. MH reports being the president of Rheumcon and receiving consulting fees from Bone Therapeutics, Bristol-Myers Squibb, Eli Lilly, Galapagos, IBSA Insititut Biotechniq SA, Novartis Pharma AG, Pfizer, Samumed LLC, Theralogix LLC and Kolon TissueGene. HG, BD, OG, CL and MM are employees of Merck KGaA, Darmstadt, Germany. FM and VO are employees of EMD Serono (a business of Merck KGaA, Darmstadt, Germany). ARB, IB and JRA are employees and shareholders in Nordic Bioscience. PGC has received consultancy or speaker’s bureau fees from AbbVie, AstraZeneca, BMS, EMD Serono (a business of Merck KGaA, Darmstadt, Germany), Flexion Therapeutics, Galapagos, Kolon Tissue-Gene, Novartis, Pfizer, Samumed and Stryker.
Figures

Comment in
-
Dual-targeted disease-modifying therapies for osteoarthritis.Lancet. 2024 Jun 15;403(10444):2591. doi: 10.1016/S0140-6736(24)00475-6. Lancet. 2024. PMID: 38879250 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
