

Clinical Outcomes in Patients with Multi-Hit TP53 Chronic Lymphocytic Leukemia Treated with Ibrutinib
- PMID: 33963002
- PMCID: PMC8364879
- DOI: 10.1158/1078-0432.CCR-20-4890
Clinical Outcomes in Patients with Multi-Hit TP53 Chronic Lymphocytic Leukemia Treated with Ibrutinib
Abstract
Purpose: TP53 aberration (TP53 mutation and/or 17p deletion) is the most important predictive marker in chronic lymphocytic leukemia (CLL). Although each TP53 aberration is considered an equal prognosticator, the prognostic value of carrying isolated (single-hit) or multiple (multi-hit) TP53 aberrations remains unclear, particularly in the context of targeted agents.
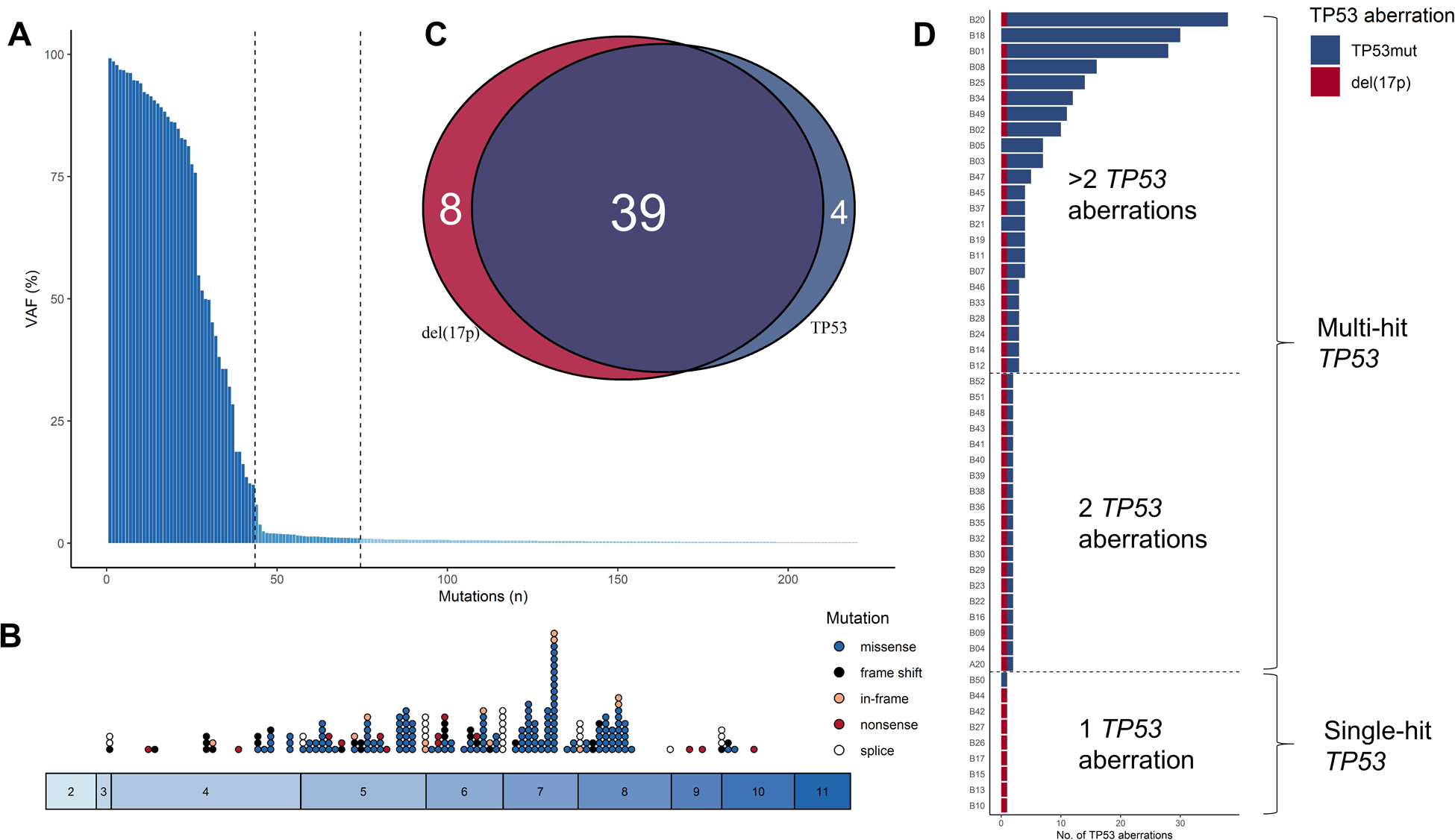
Patients and methods: We performed deep sequencing of TP53 using baseline samples collected from 51 TP53 aberrant patients treated with ibrutinib in a phase II study (NCT01500733).
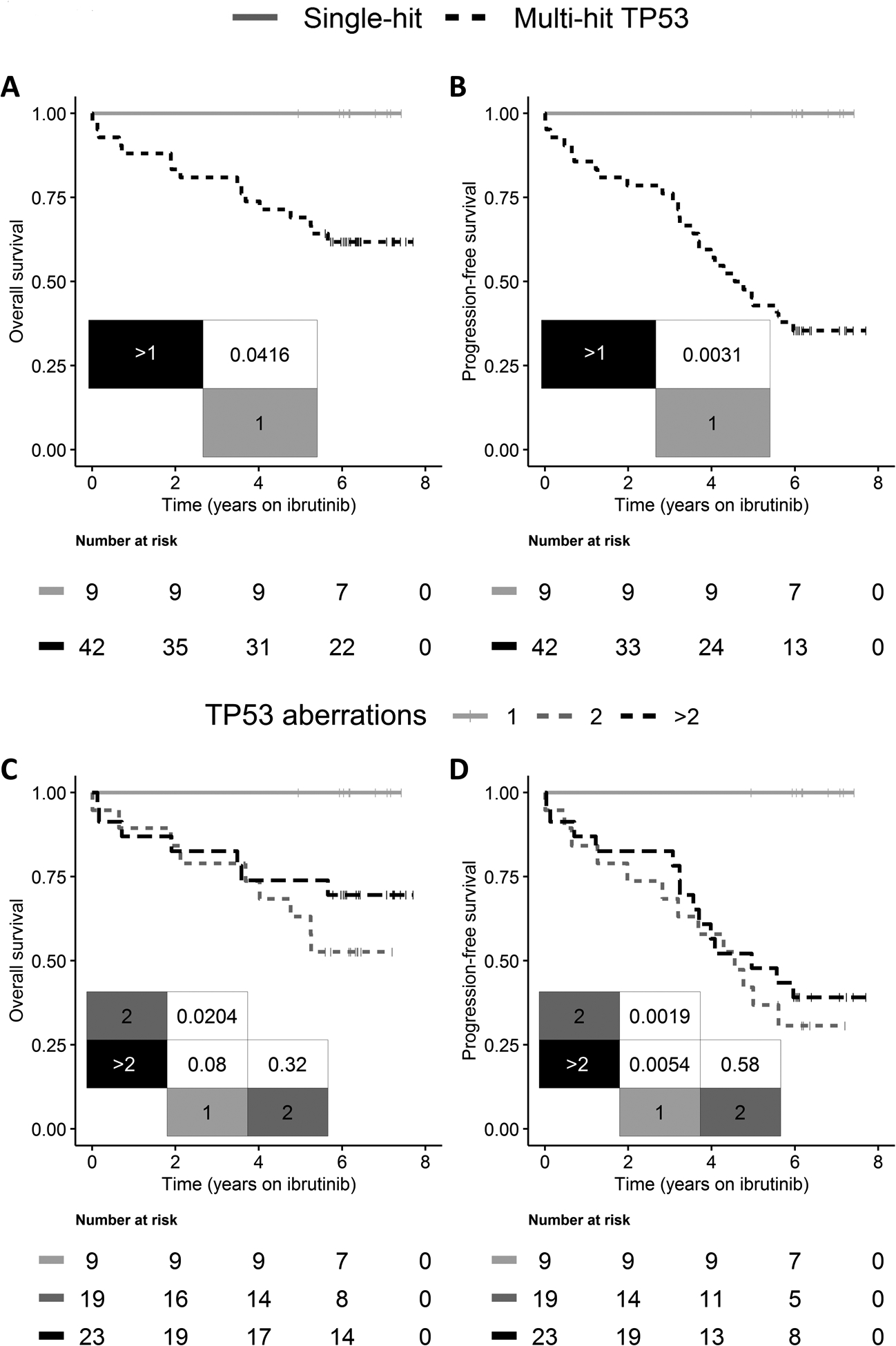
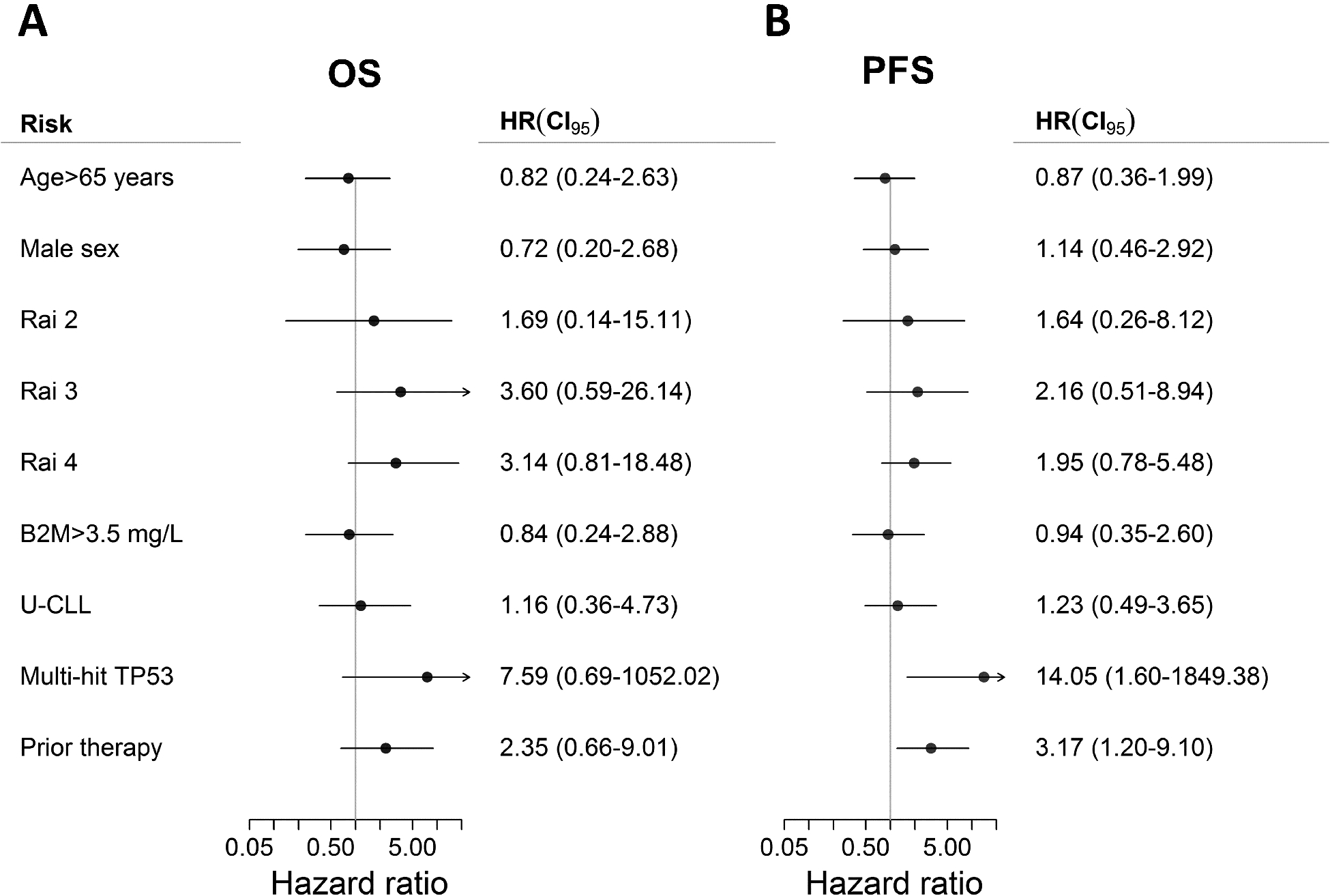
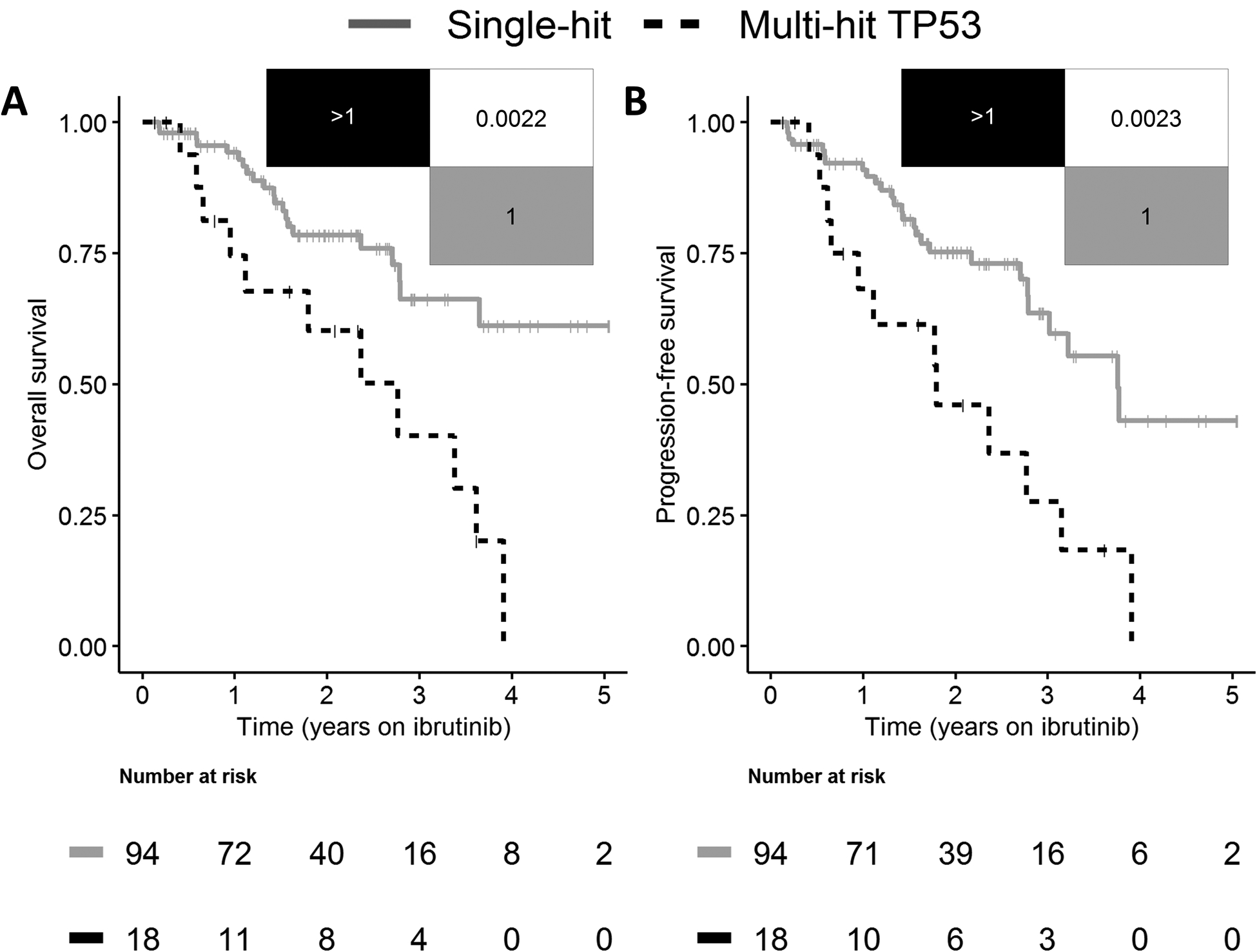
Results: We identified TP53 mutations in 43 patients (84%) and del(17p) in 47 (92%); 9 and 42 patients carried single-hit and multi-hit TP53, respectively. The multi-hit TP53 subgroup was enriched with younger patients who had prior treatments and unmutated immunoglobulin heavy-chain variable region gene status. We observed significantly shorter overall survival, progression-free survival (PFS), and time-to-progression (TTP) in patients with multi-hit TP53 compared with those with single-hit TP53. Clinical outcomes were similar in patient subgroups stratified by 2 or >2 TP53 aberrations. In multivariable analyses, multi-hit TP53 CLL was independently associated with inferior PFS and TTP. In sensitivity analyses, excluding mutations below 1% VAF demonstrated similar outcome. Results were validated in an independent population-based cohort of 112 patients with CLL treated with ibrutinib.
Conclusions: In this study, single-hit TP53 defines a distinct subgroup of patients with an excellent long-term response to single-agent ibrutinib, whereas multi-hit TP53 is independently associated with shorter PFS. These results warrant further investigations on prognostication and management of multi-hit TP53 CLL.See related commentary by Bomben et al., p. 4462.
©2021 American Association for Cancer Research.
Figures
Comment in
-
TP53 Disruption in Chronic Lymphocytic Leukemia Under Ibrutinib: More is Worse?Clin Cancer Res. 2021 Aug 15;27(16):4462-4464. doi: 10.1158/1078-0432.CCR-21-1750. Epub 2021 Jun 14. Clin Cancer Res. 2021. PMID: 34127506
References
-
- Donehower LA, Soussi T, Korkut A, Liu Y, Schultz A, Cardenas M, et al. Integrated Analysis of TP53 Gene and Pathway Alterations in The Cancer Genome Atlas. Cell reports. 2019;28:3010. - PubMed
-
- Stilgenbauer S, Schnaiter A, Paschka P, Zenz T, Rossi M, Dohner K, et al. Gene mutations and treatment outcome in chronic lymphocytic leukemia: results from the CLL8 trial. Blood. 2014;123:3247–54. - PubMed
-
- Bahlo J, Kutsch N, Bauer K, Bergmann MA, Byrd J, Chaffee KG, et al. An international prognostic index for patients with chronic lymphocytic leukaemia (CLL-IPI): a meta-analysis of individual patient data. Lancet Oncol. 2016;17:779–90. - PubMed
-
- Burger JA. Treatment of Chronic Lymphocytic Leukemia. N Engl J Med. 2020;383:460–73. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
