

Immune cell composition and functional marker dynamics from multiplexed immunohistochemistry to predict response to neoadjuvant chemotherapy in the WSG-ADAPT-TN trial
- PMID: 33963012
- PMCID: PMC8108653
- DOI: 10.1136/jitc-2020-002198
Immune cell composition and functional marker dynamics from multiplexed immunohistochemistry to predict response to neoadjuvant chemotherapy in the WSG-ADAPT-TN trial
Abstract
Background: The association of early changes in the immune infiltrate during neoadjuvant chemotherapy (NACT) with pathological complete response (pCR) in triple-negative breast cancer (TNBC) remains unexplored.
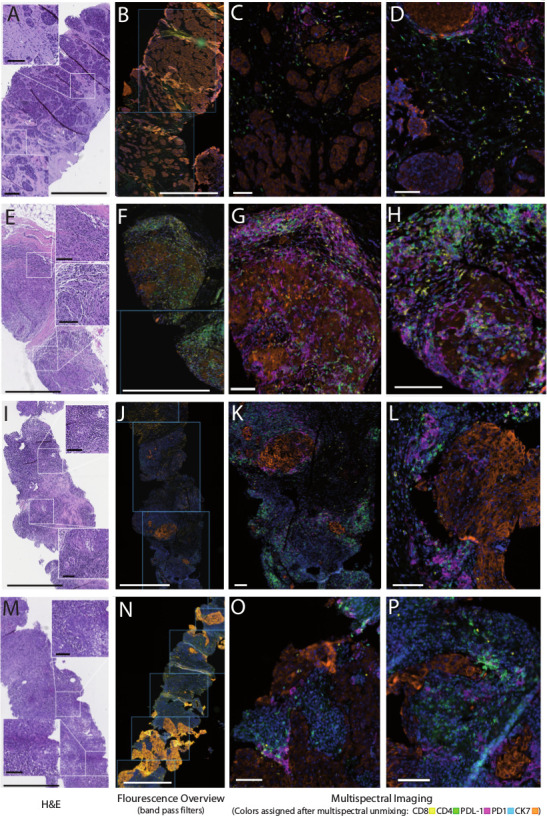
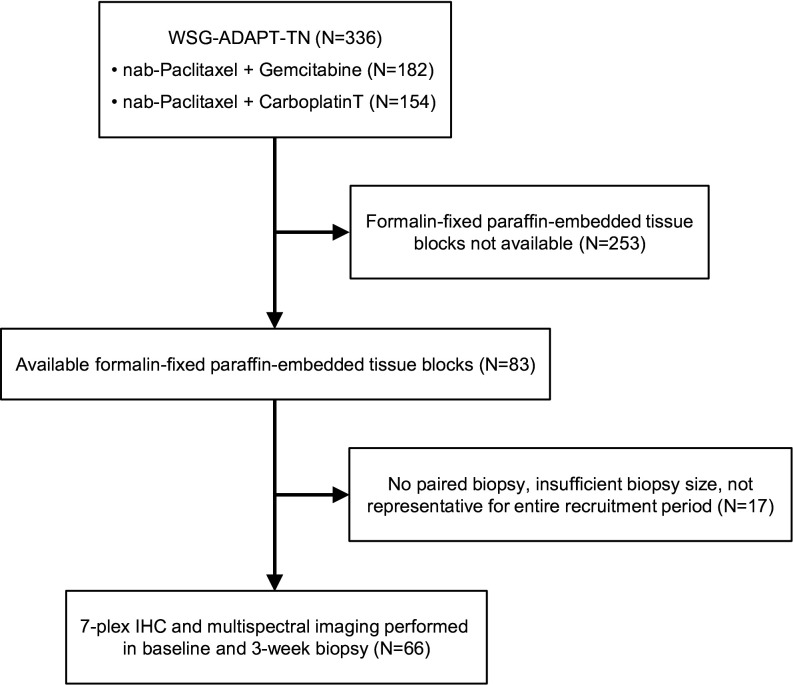
Methods: Multiplexed immunohistochemistry was performed in matched tumor biopsies obtained at baseline and after 3 weeks of NACT from 66 patients from the West German Study Group Adjuvant Dynamic Marker-Adjusted Personalized Therapy Trial Optimizing Risk Assessment and Therapy Response Prediction in Early Breast Cancer - Triple Negative Breast Cancer (WSG-ADAPT-TN) trial. Association between CD4, CD8, CD73, T cells, PD1-positive CD4 and CD8 cells, and PDL1 levels in stroma and/or tumor at baseline, week 3 and 3-week change with pCR was evaluated with univariable logistic regression.
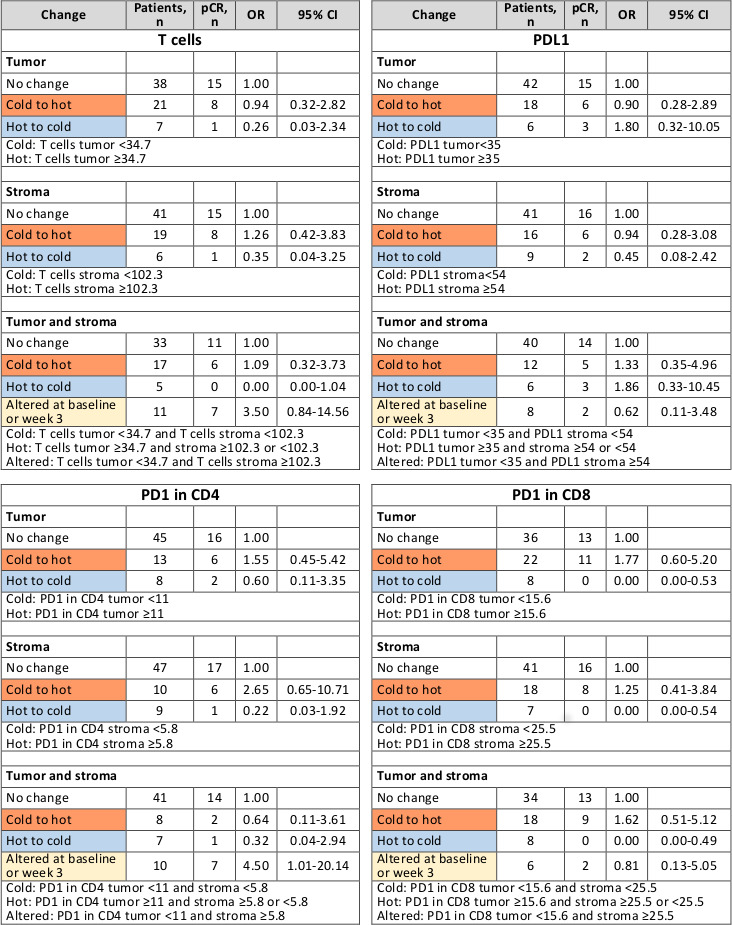
Results: Compared with no change in immune cell composition and functional markers, transition from 'cold' to 'hot' (below-median and above-median marker level at baseline, respectively) suggested higher pCR rates for PD1-positive CD4 (tumor: OR=1.55, 95% CI 0.45 to 5.42; stroma: OR=2.65, 95% CI 0.65 to 10.71) and PD1-positive CD8 infiltrates (tumor: OR=1.77, 95% CI 0.60 to 5.20; stroma: OR=1.25, 95% CI 0.41 to 3.84; tumor+stroma: OR=1.62, 95% CI 0.51 to 5.12). No pCR was observed after 'hot-to-cold' transition in PD1-positive CD8 cells. pCR rates appeared lower after hot-to-cold transitions in T cells (tumor: OR=0.26, 95% CI 0.03 to 2.34; stroma: OR=0.35, 95% CI 0.04 to 3.25; tumor+stroma: OR=0.00, 95% CI 0.00 to 1.04) and PD1-positive CD4 cells (tumor: OR=0.60, 95% CI 0.11 to 3.35; stroma: OR=0.22, 95% CI 0.03 to 1.92; tumor+stroma: OR=0.32, 95% CI 0.04 to 2.94). Higher pCR rates collated with 'altered' distribution (levels below-median and above-median in tumor and stroma, respectively) of T cell (OR=3.50, 95% CI 0.84 to 14.56) and PD1-positive CD4 cells (OR=4.50, 95% CI 1.01 to 20.14).
Conclusion: Our exploratory findings indicate that comprehensive analysis of early immune infiltrate dynamics complements currently investigated predictive markers for pCR and may have a potential to improve guidance for individualized de-escalation/escalation strategies in TNBC.
Keywords: biomarkers; breast neoplasms; immune evation; programmed cell death 1 receptor; tumor; tumor microenvironment.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials