

Lipoprotein(a) is robustly associated with aortic valve calcium
- PMID: 33963048
- PMCID: PMC8372399
- DOI: 10.1136/heartjnl-2021-319044
Lipoprotein(a) is robustly associated with aortic valve calcium
Abstract
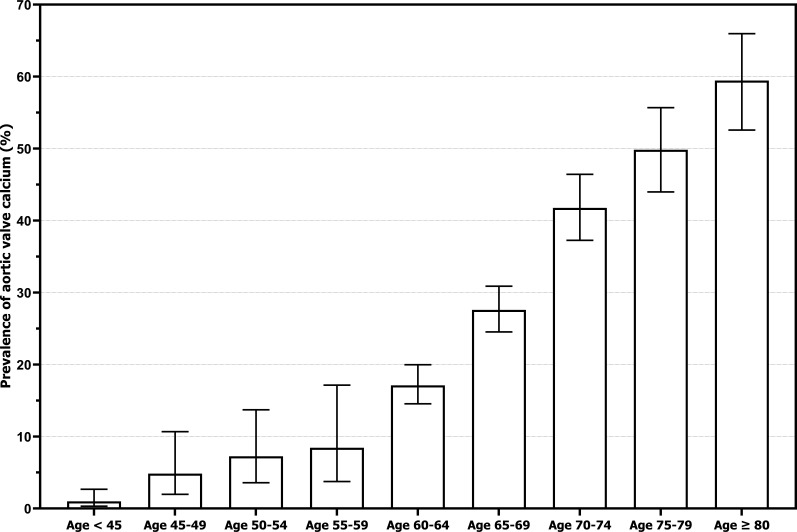
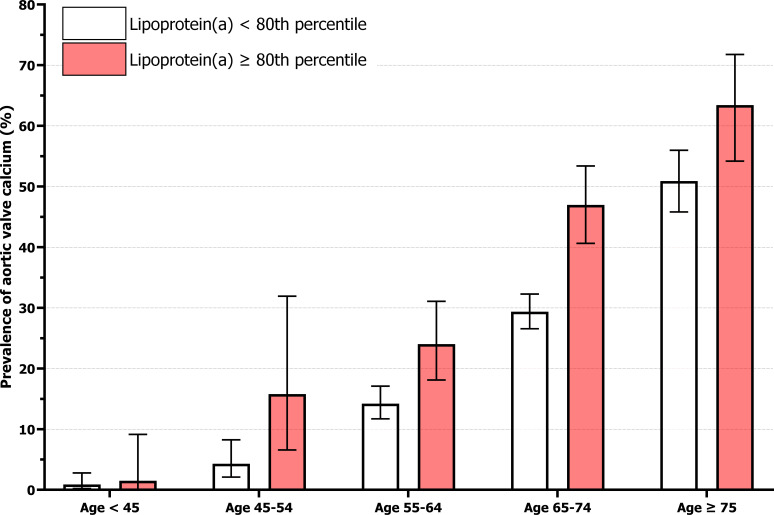
Objectives: To investigate the prevalence and quantity of aortic valve calcium (AVC) in two large cohorts, stratified according to age and lipoprotein(a) (Lp(a)), and to assess the association between Lp(a) and AVC.
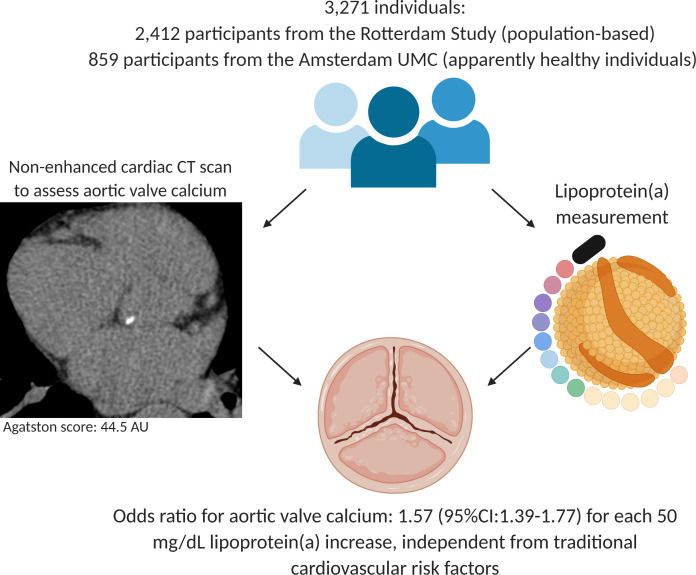
Methods: We included 2412 participants from the population-based Rotterdam Study (52% women, mean age=69.6±6.3 years) and 859 apparently healthy individuals from the Amsterdam University Medical Centers (UMC) outpatient clinic (57% women, mean age=45.9±11.6 years). All individuals underwent blood sampling to determine Lp(a) concentration and non-enhanced cardiac CT to assess AVC. Logistic and linear regression analyses were performed to investigate the associations of Lp(a) with the presence and amount of AVC.
Results: The prevalence of AVC was 33.1% in the Rotterdam Study and 5.4% in the Amsterdam UMC cohort. Higher Lp(a) concentrations were independently associated with presence of AVC in both cohorts (OR per 50 mg/dL increase in Lp(a): 1.54 (95% CI 1.36 to 1.75) in the Rotterdam Study cohort and 2.02 (95% CI 1.19 to 3.44) in the Amsterdam UMC cohort). In the Rotterdam Study cohort, higher Lp(a) concentrations were also associated with increase in aortic valve Agatston score (β 0.19, 95% CI 0.06 to 0.32 per 50 mg/dL increase).
Conclusions: Lp(a) is robustly associated with presence of AVC in a wide age range of individuals. These results provide further rationale to assess the effect of Lp(a) lowering interventions in individuals with early AVC to prevent end-stage aortic valve stenosis.
Keywords: aortic valve stenosis; hyperlipidaemias; multidetector computed tomography.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: SSS, YBdR and ES were supported by Amgen: Lp(a) Ahead Study. ESGS has received research grants/support to his institution from Amgen, Sanofi, Resverlogix and Athera, and has served as a consultant for Amgen, Sanofi, Esperion, Novartis and Ionis Pharmaceuticals.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous