

Quality of care and risk of incident atrial fibrillation in patients with newly diagnosed heart failure: a nationwide cohort study
- PMID: 33963404
- PMCID: PMC9989597
- DOI: 10.1093/ehjqcco/qcab036
Quality of care and risk of incident atrial fibrillation in patients with newly diagnosed heart failure: a nationwide cohort study
Abstract
Aims: Incident atrial fibrillation (AF) is an adverse prognostic indicator in heart failure (HF); identifying modifiable targets may be relevant to reduce the incidence and morbidity of AF. Therefore, we examined the association between quality of HF care and risk of AF.
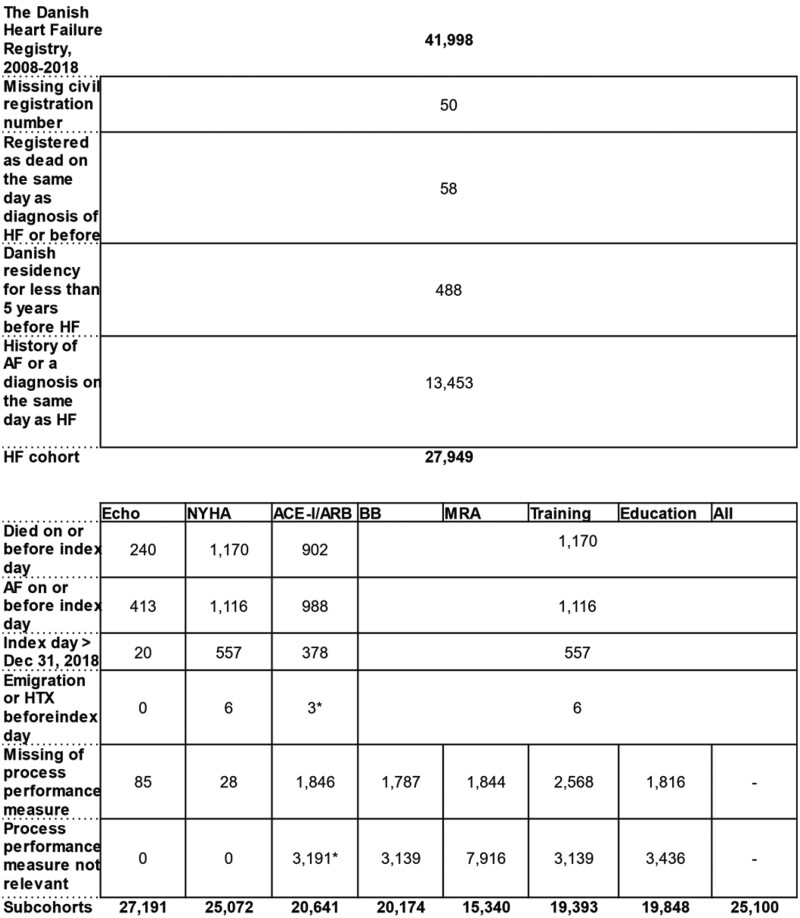
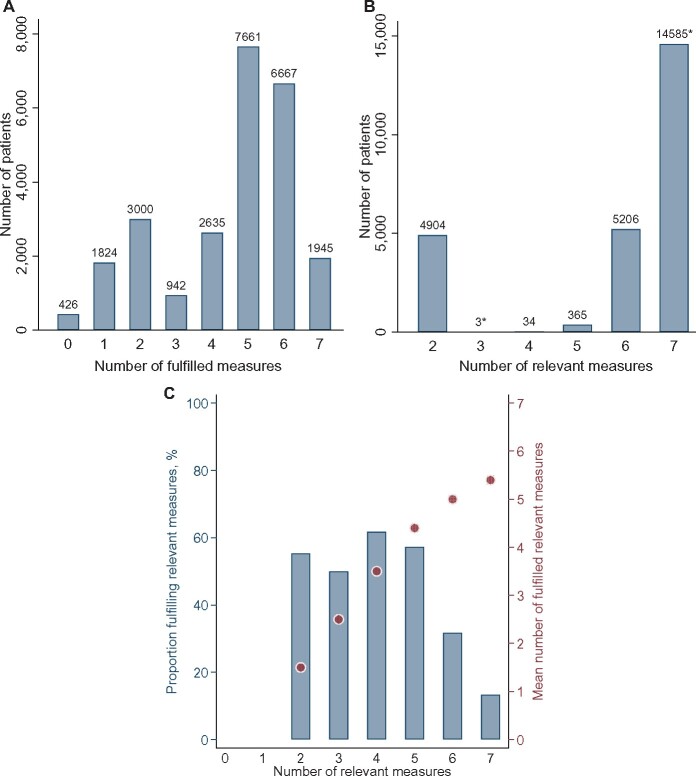
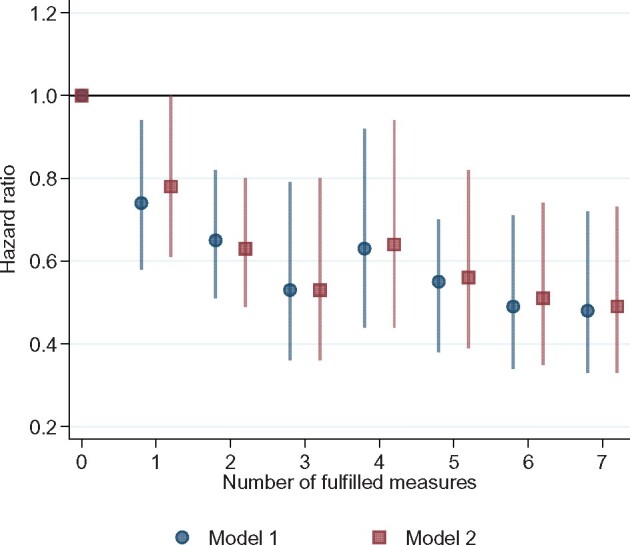
Methods and results: Using the Danish Heart Failure Registry, we conducted a nationwide registry-based cohort study of all incident HF patients diagnosed between 2008 and 2018 and without history of AF. Quality of HF care was assessed by seven process performance measures, including echocardiographic examination, New York Heart Association classification, treatment with angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers, beta-blockers, and mineralocorticoid antagonists, physical training, and patient education. In the main analysis, we examined adherence with all measures in a cohort of 25 100 patients (mean age 68.5 ± 13.2 years; 33.6% women). The median follow-up was 3.1 years. Cox proportional hazard regressions estimated the hazard ratios (HRs) with 95% confidence intervals (95% CIs) between the number of fulfilled measures and incident AF. In a multivariable-adjusted analysis with 0 fulfilled performance measures as reference, the HRs (95% CIs) were 1: 0.78 (0.61-1.00), 2: 0.63 (0.49-0.80), 3: 0.53 (0.36-0.80), 4: 0.64 (0.44-0.94), 5: 0.56 (0.39-0.82), 6: 0.51 (0.35-0.74), and 7: 0.49 (0.33-0.73), with a significant decreasing linear trend (P < 0.001).
Conclusion: In patients with incident HF, fulfilment of guideline-based process performance measures was associated with decreased long-term risk of AF. This study supports initiatives to improve the quality of care for patients with HF to prevent incident AF.
Keywords: Atrial fibrillation; Heart failure; Process performance measure; Quality indicators; Quality of health care.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2021. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Lloyd-Jones DM, Larson MG, Leip EP, Beiser A, D'Agostino RB, Kannel WB et al. Lifetime risk for developing congestive heart failure: the Framingham Heart Study. Circulation 2002;106:3068–3072. - PubMed
-
- Bleumink GS, Knetsch AM, Sturkenboom MC, Straus SM, Hofman A, Deckers JW et al. Quantifying the heart failure epidemic: prevalence, incidence rate, lifetime risk and prognosis of heart failure The Rotterdam Study. Eur Heart J 2004;25:1614–1619. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
