

Role of sleep on respiratory failure after extubation in the ICU
- PMID: 33963951
- PMCID: PMC8105690
- DOI: 10.1186/s13613-021-00863-z
Role of sleep on respiratory failure after extubation in the ICU
Abstract
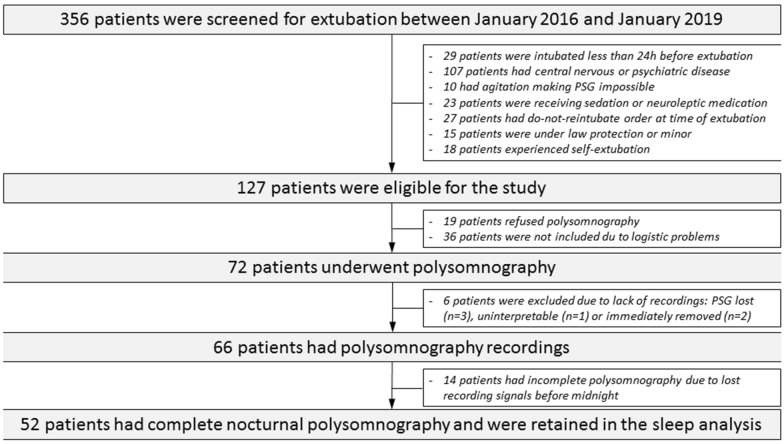
Background: Sleep had never been assessed immediately after extubation in patients still in the ICU. However, sleep deprivation may alter respiratory function and may promote respiratory failure. We hypothesized that sleep alterations after extubation could be associated with an increased risk of post-extubation respiratory failure and reintubation. We conducted a prospective observational cohort study performed at the medical ICU of the university hospital of Poitiers in France. Patients at high-risk of extubation failure (> 65 years, with any underlying cardiac or lung disease, or intubated > 7 days) were included. Patients intubated less than 24 h, with central nervous or psychiatric disorders, continuous sedation, neuroleptic medication, or uncooperative were excluded. Sleep was assessed by complete polysomnography just following extubation including the night. The main objective was to compare sleep between patients who developed post-extubation respiratory failure or required reintubation and the others.
Results: Over a 3-year period, 52 patients had complete polysomnography among whom 12 (23%) developed post-extubation respiratory failure and 8 (15%) required reintubation. Among them, 10 (19%) had atypical sleep, 15 (29%) had no deep sleep, and 33 (63%) had no rapid eye movement (REM) sleep. Total sleep time was 3.2 h in median [interquartile range, 2.0-4.4] in patients who developed post-extubation respiratory failure vs. 2.0 [1.1-3.8] in those who were successfully extubated (p = 0.34). Total sleep time, and durations of deep and REM sleep stages did not differ between patients who required reintubation and the others. Reintubation rates were 21% (7/33) in patients with no REM sleep and 5% (1/19) in patients with REM sleep (difference, - 16% [95% CI - 33% to 6%]; p = 0.23).
Conclusions: Sleep assessment by polysomnography after extubation showed a dramatically low total, deep and REM sleep time. Sleep did not differ between patients who were successfully extubated and those who developed post-extubation respiratory failure or required reintubation.
Keywords: Airway extubation; Intensive care unit; Mechanical ventilation; Sleep; Ventilator weaning.
Conflict of interest statement
AWT reported receiving grants from the French ministry of Health, personal fees (payment for lectures, and travel/accommodation expense coverage to attend scientific meetings) and non-financial support from Fisher & Paykel, GE Healthcare, Maquet–Getinge, and Covidien outside the submitted work. JPF reported receiving grants from the French Ministry of Health; grants, personal fees, and non-financial support from Fisher & Paykel Healthcare, and personal fees and non-financial support from SOS Oxygène, outside of the submitted work.
Figures



References
LinkOut - more resources
Full Text Sources
Other Literature Sources
