

A Randomized Phase 1 Safety, Pharmacokinetic and Pharmacodynamic Study of the Novel Myostatin Inhibitor Apitegromab (SRK-015): A Potential Treatment for Spinal Muscular Atrophy
- PMID: 33963971
- PMCID: PMC8189951
- DOI: 10.1007/s12325-021-01757-z
A Randomized Phase 1 Safety, Pharmacokinetic and Pharmacodynamic Study of the Novel Myostatin Inhibitor Apitegromab (SRK-015): A Potential Treatment for Spinal Muscular Atrophy
Abstract
Introduction: Apitegromab (SRK-015) is an anti-promyostatin monoclonal antibody under development to improve motor function in patients with spinal muscular atrophy, a rare neuromuscular disease. This phase 1 double-blind, placebo-controlled study assessed safety, pharmacokinetic parameters, pharmacodynamics (serum latent myostatin), and immunogenicity of single and multiple ascending doses of apitegromab in healthy adult subjects.
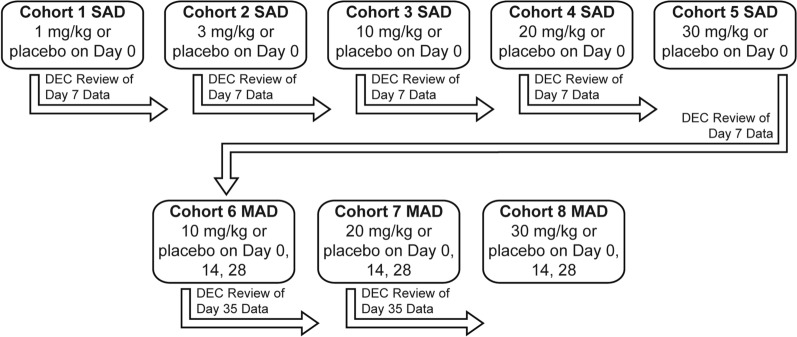
Methods: Subjects were administered single intravenous ascending doses of apitegromab of 1, 3, 10, 20, 30 mg/kg or placebo, and multiple intravenous ascending doses of apitegromab of 10, 20, 30 mg/kg or placebo.
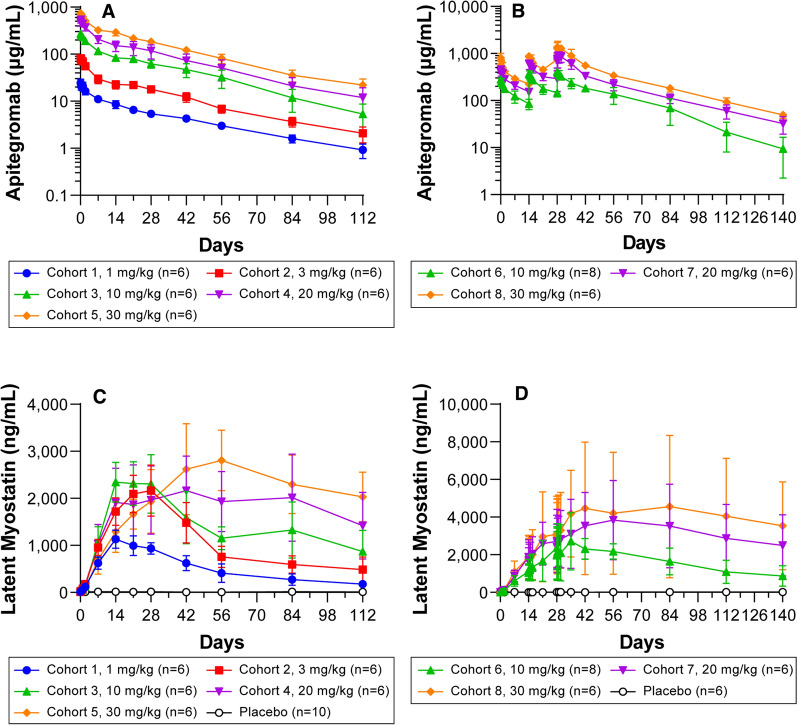
Results: Following single ascending doses, the pharmacokinetic parameters of apitegromab appeared to be similar across all dose groups, following a biphasic pattern of decline in the concentration-time curve. The mean apparent terminal t1/2 after single intravenous doses of apitegromab ranged from 24 to 31 days across dose groups. Dose-related increases were observed in Cmax following multiple ascending doses. Single and multiple apitegromab doses resulted in dose-dependent and sustained increases in serum latent myostatin, indicating robust target engagement. Apitegromab was safe and well tolerated, on the basis of the adverse event (AE) profile with no clinically meaningful changes in baseline vital signs, electrocardiograms, or clinical laboratory parameters and no anti-drug antibody formation.
Conclusion: These results support continued investigation of apitegromab for the treatment of patients with milder forms (type 2 and 3) of spinal muscular atrophy.
Keywords: Apitegromab; Human monoclonal antibody; Myostatin; Pharmacodynamics; Pharmacokinetics; Phase 1 study; SRK-015; Safety; Spinal muscular atrophy; Tolerability.
Figures
References
-
- Health and Resources and Services Administration. Newborn screening for spinal muscular atrophy. A summary of the evidence and advisory committee decision. March 13, 2018. https://www.hrsa.gov/sites/default/files/hrsa/advisory-committees/herita.... Accessed Jul 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
