

Pediatric asthma incidence rates in the United States from 1980 to 2017
- PMID: 33964299
- PMCID: PMC8631308
- DOI: 10.1016/j.jaci.2021.04.027
Pediatric asthma incidence rates in the United States from 1980 to 2017
Abstract
Background: Few studies have examined longitudinal asthma incidence rates (IRs) from a public health surveillance perspective.
Objective: Our aim was to calculate descriptive asthma IRs in children over time with consideration for demographics and parental asthma history.
Methods: Data from 9 US birth cohorts were pooled into 1 population covering the period from 1980 to 2017. The outcome was earliest parental report of a doctor diagnosis of asthma. IRs per 1,000 person-years were calculated.
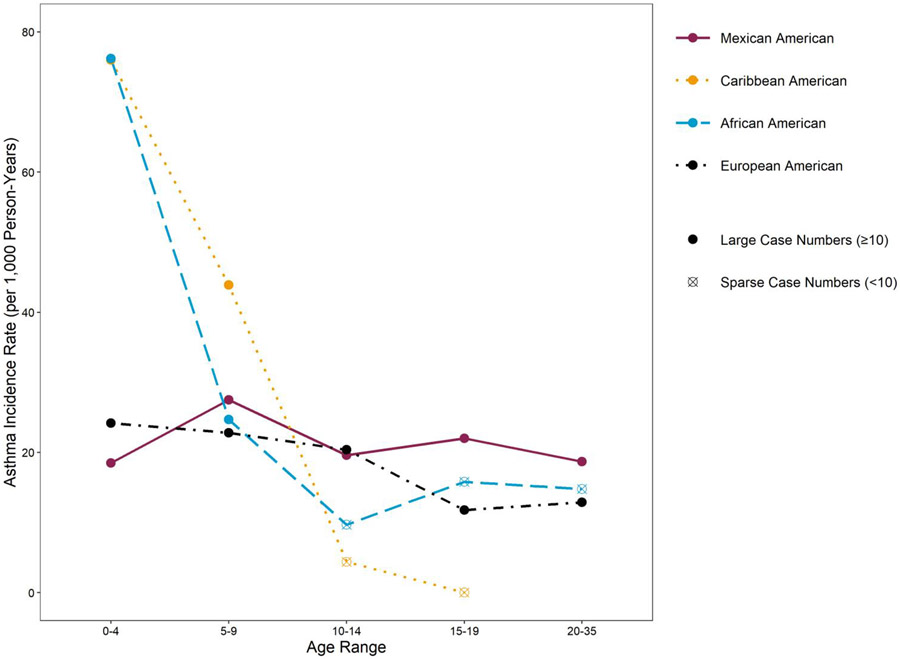
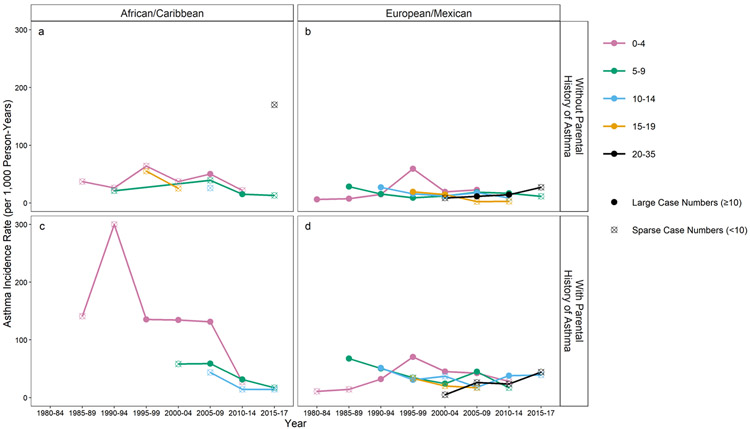
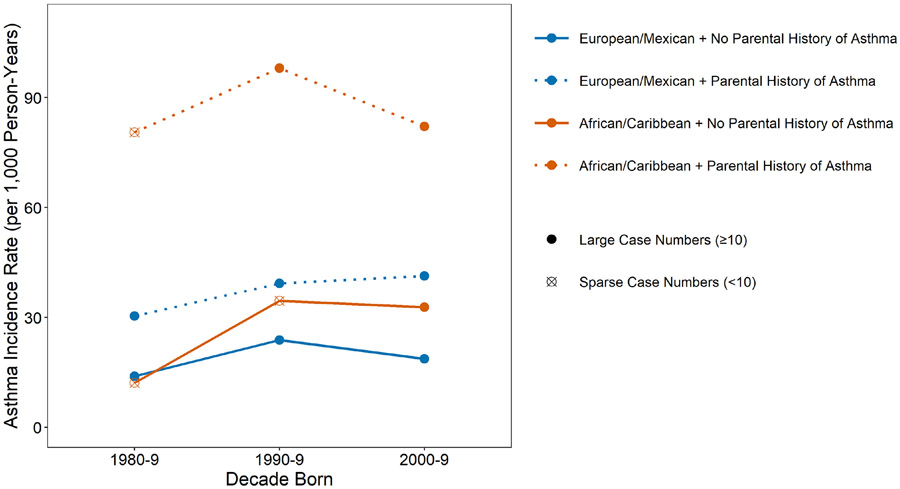
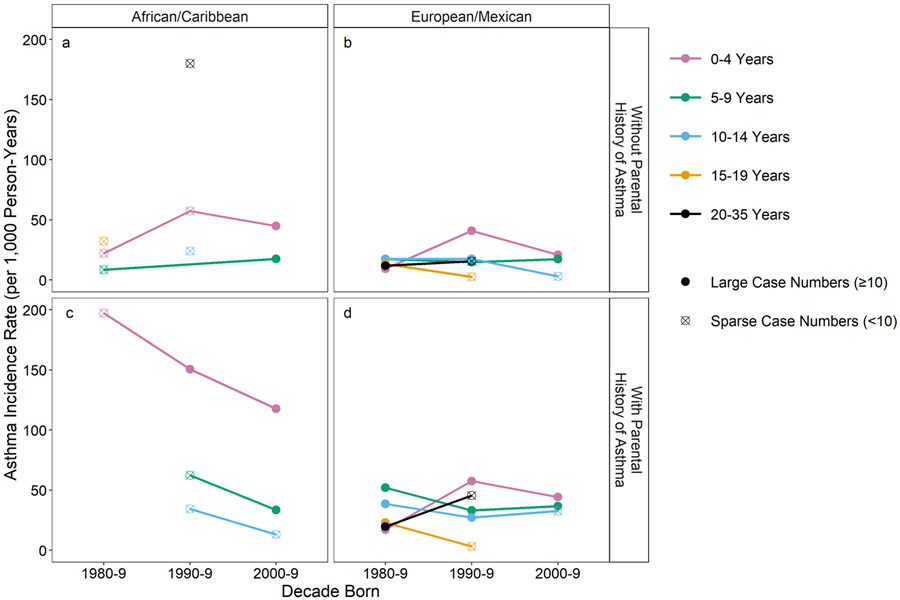
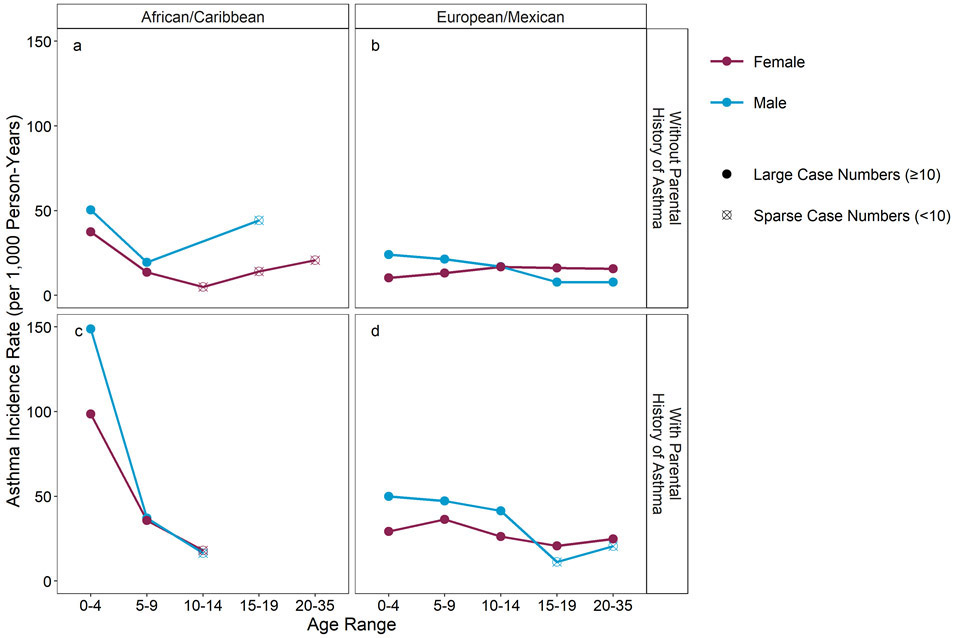
Results: The racial/ethnic backgrounds of the 6,283 children studied were as follows: 55% European American (EA), 25.5% African American (AA), 9.5% Mexican-Hispanic American (MA) and 8.5% Caribbean-Hispanic American (CA). The average follow-up was 10.4 years (SD = 8.5 years; median = 8.4 years), totaling 65,291 person-years, with 1789 asthma diagnoses yielding a crude IR of 27.5 per 1,000 person-years (95% CI = 26.3-28.8). Age-specific rates were highest among children aged 0 to 4 years, notably from 1995 to 1999, with a decline in EA and MA children in 2000 to 2004 followed by a decline in AA and CA children in 2010 to 2014. Parental asthma history was associated with statistically significantly increased rates. IRs were similar and higher in AA and CA children versus lower but similar in EA and MA children. The differential rates by sex from birth through adolescence principally resulted from a decline in rates among males but relatively stable rates among females.
Conclusions: US childhood asthma IRs varied dramatically by age, sex, parental asthma history, race/ethnicity, and calendar year. Higher rates in the 0- to 4-year-olds group, particularly among AA/CA males with a parental history of asthma, as well as changes in rates over time and by demographic factors, suggest that asthma is driven by complex interactions between genetic susceptibility and variation in time-dependent environmental and social factors.
Keywords: Epidemiology; IRs; United States; parental history; pediatric asthma; sex; time.
Copyright © 2021 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
This content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. None of the authors reports a conflict of interest.
Figures
References
-
- Bonita R, Beaglehole R, Kjellstrom T. Basic Epidemiology. Geneva, Switzerland: World Health Organization; 2006.
-
- MacMahon B, Pugh TF. Epidemiology: Principles and Methods. Boston, MA: Little, Brown and Company; 1970.
-
- Broder I, Higgins MW, Mathews KP, Keller JB. Epidemiology of asthma and allergic rhinitis in a total community, tecumseh, Michigan.IV . Natural history. Journal of Allergy and Clinical Immunology 1974; 54:100–10. - PubMed
-
- Broder I, Higgins MW, Mathews KP, Keller JB. Epidemiology of asthma and allergic rhinitis in a total community, Tecumseh, Michigan. 3. Second survey of the community. Journal of Allergy and Clinical Immunology 1974; 53:127–38. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 AI061774/AI/NIAID NIH HHS/United States
- P01 ES009600/ES/NIEHS NIH HHS/United States
- N01 AI025496/AI/NIAID NIH HHS/United States
- UH3 OD023290/OD/NIH HHS/United States
- R21 AI059415/AI/NIAID NIH HHS/United States
- R01 ES008977/ES/NIEHS NIH HHS/United States
- UM1 AI114271/AI/NIAID NIH HHS/United States
- U10 HL064305/HL/NHLBI NIH HHS/United States
- R01 HL132523/HL/NHLBI NIH HHS/United States
- U19 AI095227/AI/NIAID NIH HHS/United States
- HHSN272200900052C/AI/NIAID NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- R01 AI035786/AI/NIAID NIH HHS/United States
- R56 AI050681/AI/NIAID NIH HHS/United States
- R01 DK113003/DK/NIDDK NIH HHS/United States
- P30 ES006694/ES/NIEHS NIH HHS/United States
- R01 AI110450/AI/NIAID NIH HHS/United States
- R21 ES022321/ES/NIEHS NIH HHS/United States
- R01 HL113010/HL/NHLBI NIH HHS/United States
- R01 ES019890/ES/NIEHS NIH HHS/United States
- M01 RR000533/RR/NCRR NIH HHS/United States
- N01 AI025482/AI/NIAID NIH HHS/United States
- R21 AI069271/AI/NIAID NIH HHS/United States
- UL1 RR024156/RR/NCRR NIH HHS/United States
- UM2 AI117870/AI/NIAID NIH HHS/United States
- UL1 RR025771/RR/NCRR NIH HHS/United States
- UH3 OD023282/OD/NIH HHS/United States
- K01 AI070606/AI/NIAID NIH HHS/United States
- R01 HL141845/HL/NHLBI NIH HHS/United States
- UL1 RR024992/RR/NCRR NIH HHS/United States
- R03 HD067427/HD/NICHD NIH HHS/United States
- R01 AI021256/AI/NIAID NIH HHS/United States
- M01 RR000071/RR/NCRR NIH HHS/United States
- R21 AI080066/AI/NIAID NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- R01 MH061879/MH/NIMH NIH HHS/United States
- UG3 OD023282/OD/NIH HHS/United States
- R01 ES011170/ES/NIEHS NIH HHS/United States
- P01 AI089473/AI/NIAID NIH HHS/United States
- R01 AI050681/AI/NIAID NIH HHS/United States
- P01 AI148104/AI/NIAID NIH HHS/United States
- R01 ES013163/ES/NIEHS NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- P01 HL070831/HL/NHLBI NIH HHS/United States
- HHSN272201000052I/AI/NIAID NIH HHS/United States
- UL1 TR002345/TR/NCATS NIH HHS/United States
- R01 HD061879/HD/NICHD NIH HHS/United States
- R01 HL056177/HL/NHLBI NIH HHS/United States
- R01 AI051598/AI/NIAID NIH HHS/United States
- UG3 OD023290/OD/NIH HHS/United States
- UL1 TR003098/TR/NCATS NIH HHS/United States
- P30 ES009089/ES/NIEHS NIH HHS/United States
- R01 HD082147/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
