

Mortality after in-hospital cardiac arrest in patients with COVID-19: A systematic review and meta-analysis
- PMID: 33964332
- PMCID: PMC8098036
- DOI: 10.1016/j.resuscitation.2021.04.025
Mortality after in-hospital cardiac arrest in patients with COVID-19: A systematic review and meta-analysis
Abstract
Aim: To estimate the mortality rate, the rate of return of spontaneous circulation (ROSC) and survival with favorable neurological outcome in patients with COVID-19 after in-hospital cardiac arrest (IHCA) and attempted cardiopulmonary resuscitation (CPR).
Methods: PubMed, EMBASE, Web of Science, bioRxiv and medRxiv were surveyed up to 8th February 2021 for studies reporting data on mortality of patients with COVID-19 after IHCA. The primary outcome sought was mortality (in-hospital or at 30 days) after IHCA with attempted CPR. Additional outcomes were the overall rate of IHCA, the rate of non-shockable presenting rhythms, the rate of ROSC and the rate of survival with favorable neurological status.
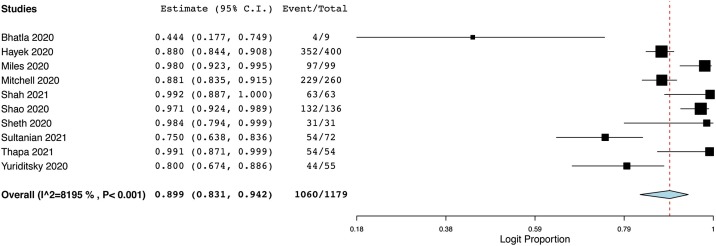
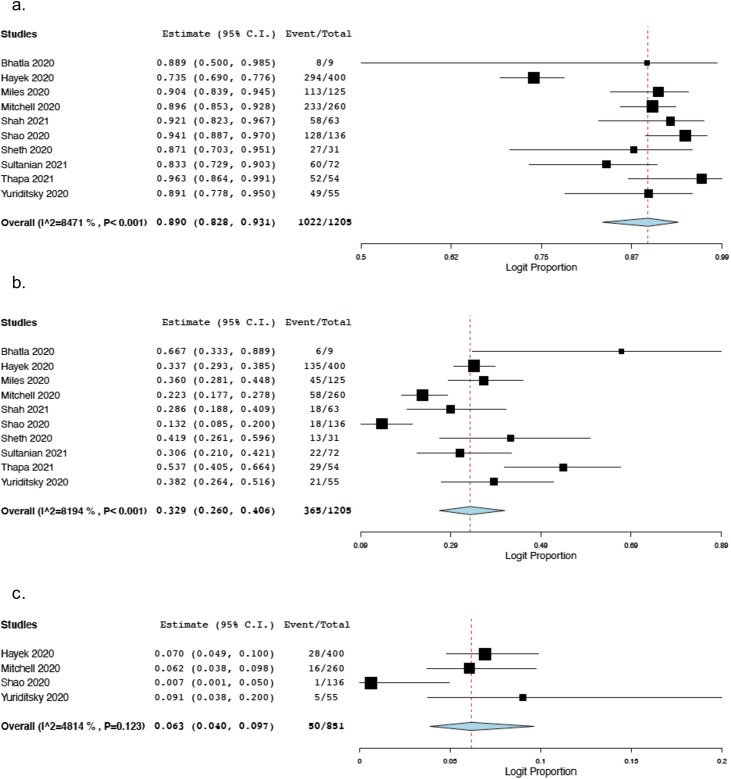
Results: Ten articles were included in the systematic review and meta-analysis, for a total of 1179 COVID-19 patients after IHCA with attempted CPR. The estimated overall mortality rate (in-hospital or at 30 days) was 89.9% (95% Predicted Interval [P.I.] 83.1%-94.2%; 1060/1179 patients; I2 = 82%). The estimated rate of non-shockable presenting rhythms was 89% (95% P.I. 82.8%-93.1%; 1022/1205 patients; I2 = 85%), and the estimated rate of ROSC was 32.9% (95% P.I. 26%-40.6%; 365/1205 patients; I2 = 82%). The estimated overall rate of survival with favorable neurological status at 30 days was 6.3% (95% P.I. 4%-9.7%; 50/851 patients; I2 = 48%). Sensitivity analysis showed that COVID-19 patients had higher risk of death after IHCA than non COVID-19 patients (OR 2.34; 95% C.I. 1.37-3.99; number of studies = 3; 1215 patients).
Conclusions: Although one of three COVID-19 patients undergoing IHCA may achieve ROSC, almost 90% may not survive at 30 days or to hospital discharge.
Keywords: COVID-19; Cardiac arrest; Mortality; cpr.
Copyright © 2021 Elsevier B.V. All rights reserved.
Figures
Comment in
-
Treating patients with ReSPECT during a pandemic: Resuscitation decisions during COVID-19.Resuscitation. 2021 Jul;164:147-148. doi: 10.1016/j.resuscitation.2021.05.024. Epub 2021 Jun 2. Resuscitation. 2021. PMID: 34089773 Free PMC article. No abstract available.
References
-
- Poissy J., Goutay J., Caplan M., et al. Pulmonary embolism in patients with COVID-19: awareness of an increased prevalence. Circulation. 2020;142:184–186. - PubMed
-
- Vicentini A., Masiello L., D’Amore S., et al. QTc interval and mortality in a population of SARS-2-CoV infected patients. Circ Arrhythm Electrophysiol. 2020;13 - PubMed
-
- University of Oxford. Coronavirus (COVID-19) Hospitalizations – Statistics and Research – Our World in Data. (Accessed 20 February 2021, at https://ourworldindata.org/covid-hospitalizations).
-
- Shah P., Smith H., Olarewaju A., et al. Is cardiopulmonary resuscitation futile in coronavirus disease 2019 patients experiencing in-hospital cardiac arrest? Crit Care Med. 2021;49:201–208. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
