

Pancreaticoduodenectomy for hepatic portal lymph node metastasis after hepatic resection for hepatocellular carcinoma: A clinical case report
- PMID: 33964712
- PMCID: PMC8121700
- DOI: 10.1016/j.ijscr.2021.105921
Pancreaticoduodenectomy for hepatic portal lymph node metastasis after hepatic resection for hepatocellular carcinoma: A clinical case report
Abstract
Introduction: In 2018, Hepatocellular carcinoma (HCC) was predicted to be the sixth most commonly diagnosed cancer. Extra-hepatic metastasis due to HCC is a poor prognostic factor, depending on the stage of the disease.
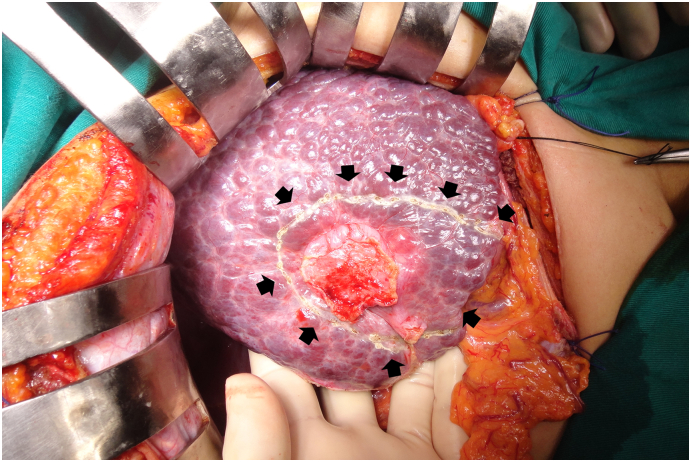
Presentation of case: We report a case of a 52-years old male who had undergone Segment 5 (S5) hepatectomy for HCC of 4.7 × 2 cm. Transcatheter arterial chemoembolization (TACE) four times postoperatively was performed based on a preoperative diagnosis of a recurrent tumour at the S1. After 2 years, the solitary tumour (7.5 × 2.5 × 3.5 cm) is located behind the right lobe of the liver and the head of the pancreas. The tumour was abnormally supplied with blood from the superior mesenteric artery (SMA) and the gastroduodenal artery (GDA). The patient was underwent pancreaticoduodenectomy (PD) to remove a large tumour. Postoperative pathology and immunohistochemical staining showed metastatic HCC. There was no tumour recurrence after 6 months.
Discussion: The organs in the body that liver cancer cells most often spread to are the lungs (44%), the portal vein (35%), the hepatobiliary ganglion (27%), and a small number of cases of bone, eye socket, bronchus metastases. Otherwise, recurrence of lymph nodes (LNs) after hepatectomy for HCC is very rare.
Conclusions: HCC can metastasize to the hepatic pedicle LN after hepatectomy and maybe confused with recurrent liver tumours in the S1. Indications for PD are feasible for solitary metastatic at peri-pancreas. Pathology incorporating immunohistochemistry can determine the origin of metastases.
Keywords: Case report; Hepatocellular carcinoma; Liver resection; Lymph node; Metastasis; Pancreatic head; Pancreaticoduodenectomy.
Copyright © 2021 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
All authors have no conflict of interest about this study.
Figures






References
-
- Bray F., Ferlay J., Soerjomataram I., Siegel R.L., Torre L.A., Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018;68(6):394–424. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
