

The performance of the Dutch Safety Management System frailty tool to predict the risk of readmission or mortality in older hospitalised cardiac patients
- PMID: 33964888
- PMCID: PMC8105911
- DOI: 10.1186/s12877-021-02243-5
The performance of the Dutch Safety Management System frailty tool to predict the risk of readmission or mortality in older hospitalised cardiac patients
Abstract
Background: Early identification of older cardiac patients at high risk of readmission or mortality facilitates targeted deployment of preventive interventions. In the Netherlands, the frailty tool of the Dutch Safety Management System (DSMS-tool) consists of (the risk of) delirium, falling, functional impairment, and malnutrition and is currently used in all older hospitalised patients. However, its predictive performance in older cardiac patients is unknown.
Aim: To estimate the performance of the DSMS-tool alone and combined with other predictors in predicting hospital readmission or mortality within 6 months in acutely hospitalised older cardiac patients.
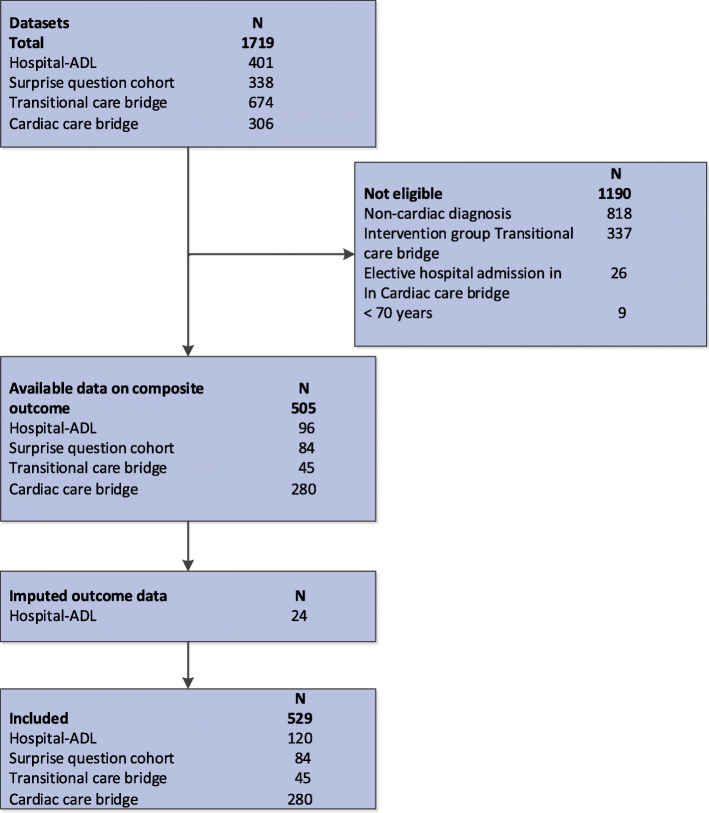
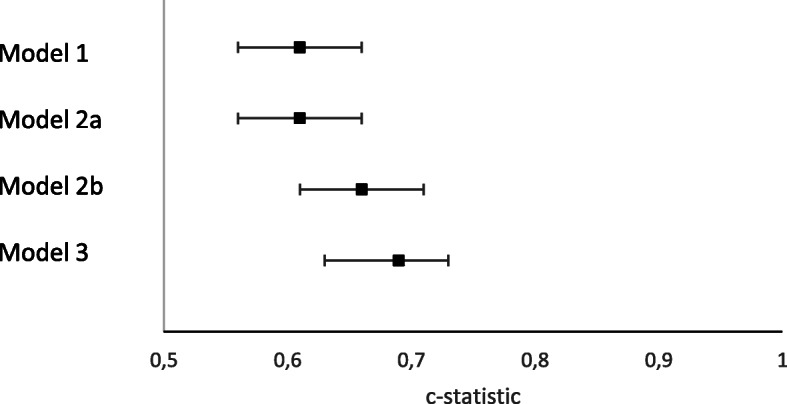
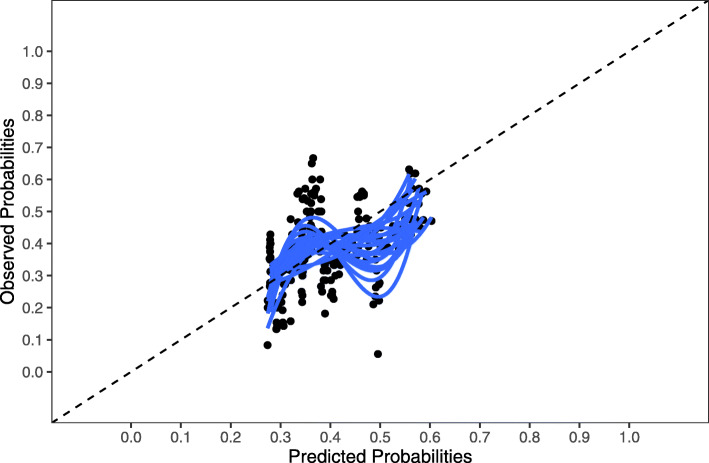
Methods: An individual patient data meta-analysis was performed on 529 acutely hospitalised cardiac patients ≥70 years from four prospective cohorts. Missing values for predictor and outcome variables were multiply imputed. We explored discrimination and calibration of: (1) the DSMS-tool alone; (2) the four components of the DSMS-tool and adding easily obtainable clinical predictors; (3) the four components of the DSMS-tool and more difficult to obtain predictors. Predictors in model 2 and 3 were selected using backward selection using a threshold of p = 0.157. We used shrunk c-statistics, calibration plots, regression slopes and Hosmer-Lemeshow p-values (PHL) to describe predictive performance in terms of discrimination and calibration.
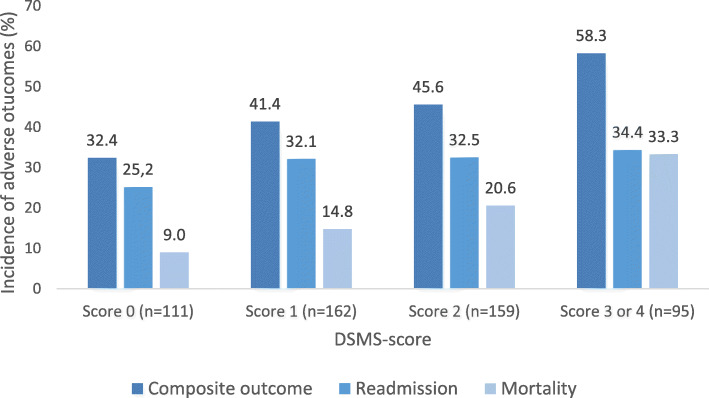
Results: The population mean age was 82 years, 52% were males and 51% were admitted for heart failure. DSMS-tool was positive in 45% for delirium, 41% for falling, 37% for functional impairments and 29% for malnutrition. The incidence of hospital readmission or mortality gradually increased from 37 to 60% with increasing DSMS scores. Overall, the DSMS-tool discriminated limited (c-statistic 0.61, 95% 0.56-0.66). The final model included the DSMS-tool, diagnosis at admission and Charlson Comorbidity Index and had a c-statistic of 0.69 (95% 0.63-0.73; PHL was 0.658).
Discussion: The DSMS-tool alone has limited capacity to accurately estimate the risk of readmission or mortality in hospitalised older cardiac patients. Adding disease-specific risk factor information to the DSMS-tool resulted in a moderately performing model. To optimise the early identification of older hospitalised cardiac patients at high risk, the combination of geriatric and disease-specific predictors should be further explored.
Keywords: Aged; Cardiovascular diseases; Frailty; Mortality; Patient readmission; Predictive value of tests; Risk assessment.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Frailty screening in hospitalised older adults: How does the brief Dutch National Safety Management Program perform compared to a more extensive approach?J Clin Nurs. 2020 Apr;29(7-8):1064-1073. doi: 10.1111/jocn.15148. Epub 2020 Jan 20. J Clin Nurs. 2020. PMID: 31856316
-
Optimal screening for increased risk for adverse outcomes in hospitalised older adults.Age Ageing. 2015 Mar;44(2):239-44. doi: 10.1093/ageing/afu187. Epub 2014 Nov 28. Age Ageing. 2015. PMID: 25432981 Free PMC article.
-
Thirty-Day Readmission Risk Model for Older Adults Hospitalized With Acute Myocardial Infarction.Circ Cardiovasc Qual Outcomes. 2019 May;12(5):e005320. doi: 10.1161/CIRCOUTCOMES.118.005320. Circ Cardiovasc Qual Outcomes. 2019. PMID: 31010300 Free PMC article.
-
Value of the Safety Management System (VMS) frailty instrument as a frailty screener in care for older hospital patients: a systematic review.Eur Geriatr Med. 2024 Jun;15(3):609-620. doi: 10.1007/s41999-024-00957-4. Epub 2024 Apr 26. Eur Geriatr Med. 2024. PMID: 38668846 Free PMC article.
-
Frailty as a predictor of all-cause mortality and readmission in older patients with acute coronary syndrome : A systematic review and meta-analysis.Wien Klin Wochenschr. 2020 Jun;132(11-12):301-309. doi: 10.1007/s00508-020-01650-9. Epub 2020 Apr 27. Wien Klin Wochenschr. 2020. PMID: 32342196
Cited by
-
Association of Vulnerability Screening on Hospital Admission with Discharge to Rehabilitation-Oriented Care after Acute Hospital Stay.Ann Geriatr Med Res. 2023 Dec;27(4):301-309. doi: 10.4235/agmr.23.0068. Epub 2023 Sep 11. Ann Geriatr Med Res. 2023. PMID: 37691483 Free PMC article.
-
Issues and Challenges of Older Persons and Research and Health Facility-based Assessors in the Conduct of Comprehensive Geriatric Assessment in the Philippines: A Descriptive Study.Acta Med Philipp. 2025 Jun 30;59(8):52-64. doi: 10.47895/amp.vi0.10258. eCollection 2025. Acta Med Philipp. 2025. PMID: 40755563 Free PMC article.
-
Age‑adjusted Charlson comorbidity index and in‑hospital mortality in critically ill patients with cardiogenic shock: A retrospective cohort study.Exp Ther Med. 2023 May 5;25(6):299. doi: 10.3892/etm.2023.11998. eCollection 2023 Jun. Exp Ther Med. 2023. PMID: 37229315 Free PMC article.
References
-
- Jepma P, Ter Riet G, van Rijn M, Latour CHM, Peters RJG, WJM SOR, et al. Readmission and mortality in patients >/=70 years with acute myocardial infarction or heart failure in the Netherlands: a retrospective cohort study of incidences and changes in risk factors over time. Neth Heart J. 2019;27(3):134–141. doi: 10.1007/s12471-019-1227-4. - DOI - PMC - PubMed
-
- Gorodeski EZ, Goyal P, Hummel SL, Krishnaswami A, Goodlin SJ, Hart LL, Forman DE, Wenger NK, Kirkpatrick JN, Alexander KP, Geriatric Cardiology Section Leadership Council, American College of Cardiology Domain management approach to heart failure in the geriatric patient: present and future. J Am Coll Cardiol. 2018;71(17):1921–1936. doi: 10.1016/j.jacc.2018.02.059. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
