

Variants and Pitfalls in PET/CT Imaging of Gastrointestinal Cancers
- PMID: 33965198
- PMCID: PMC8338802
- DOI: 10.1053/j.semnuclmed.2021.04.001
Variants and Pitfalls in PET/CT Imaging of Gastrointestinal Cancers
Abstract
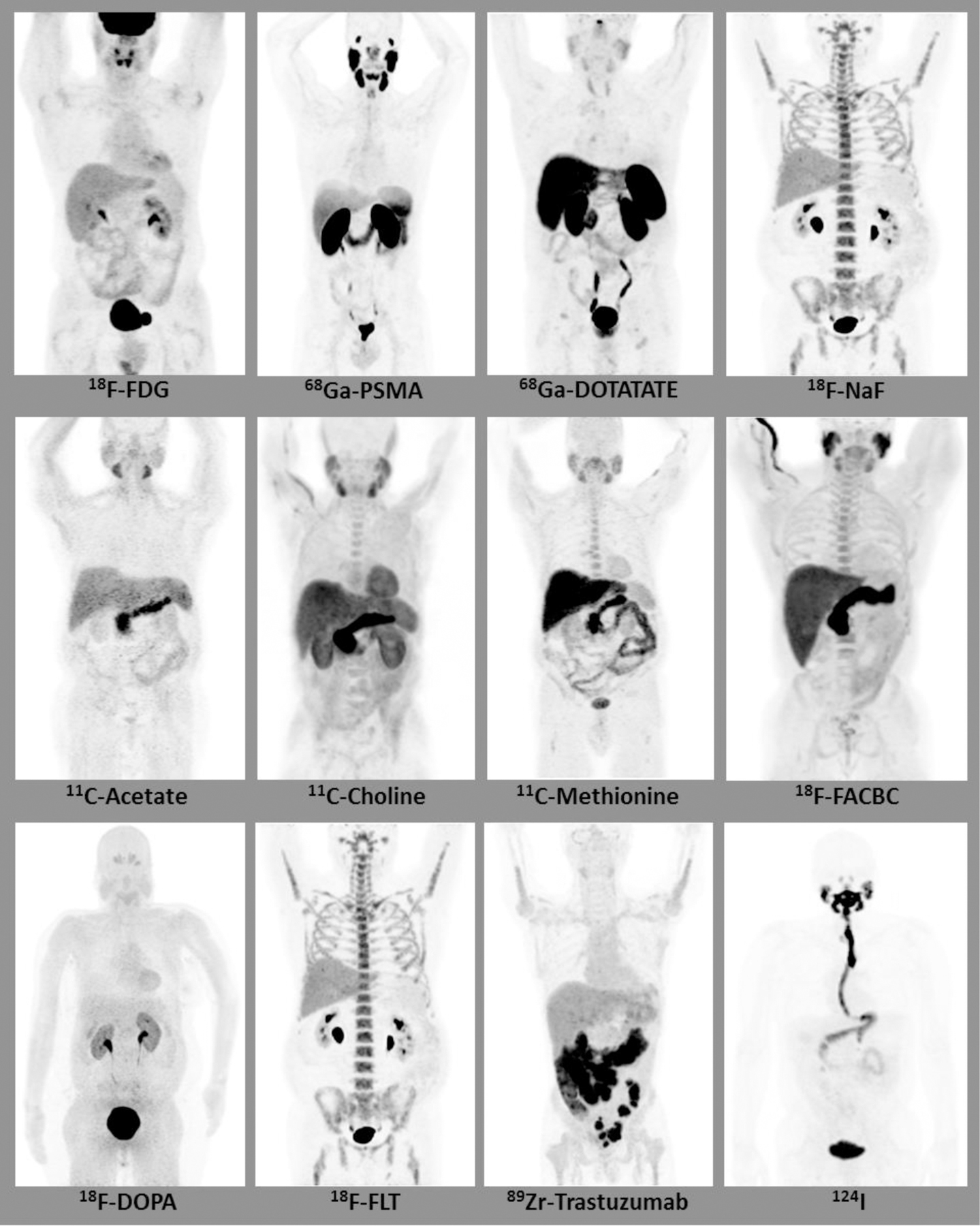
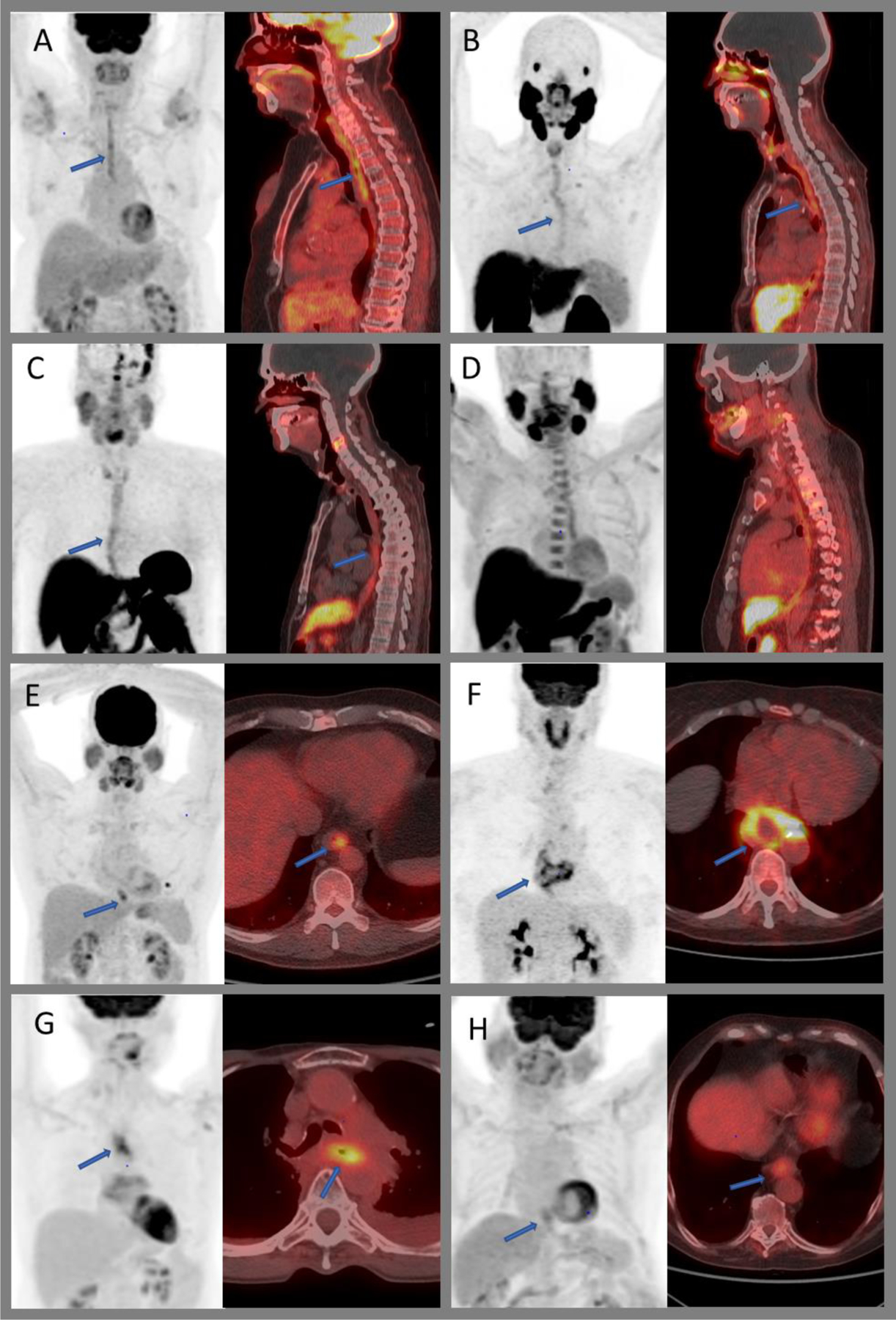
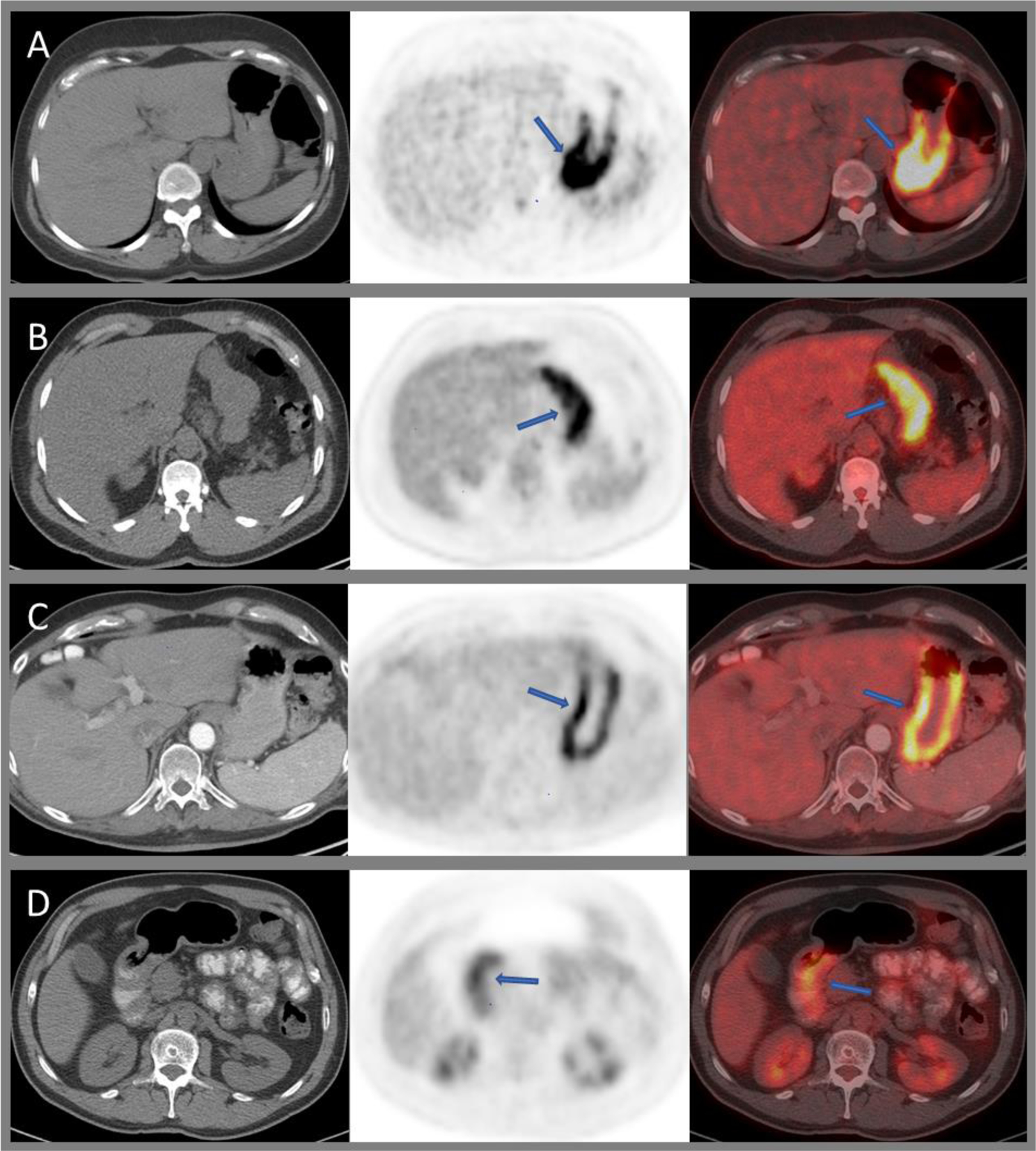
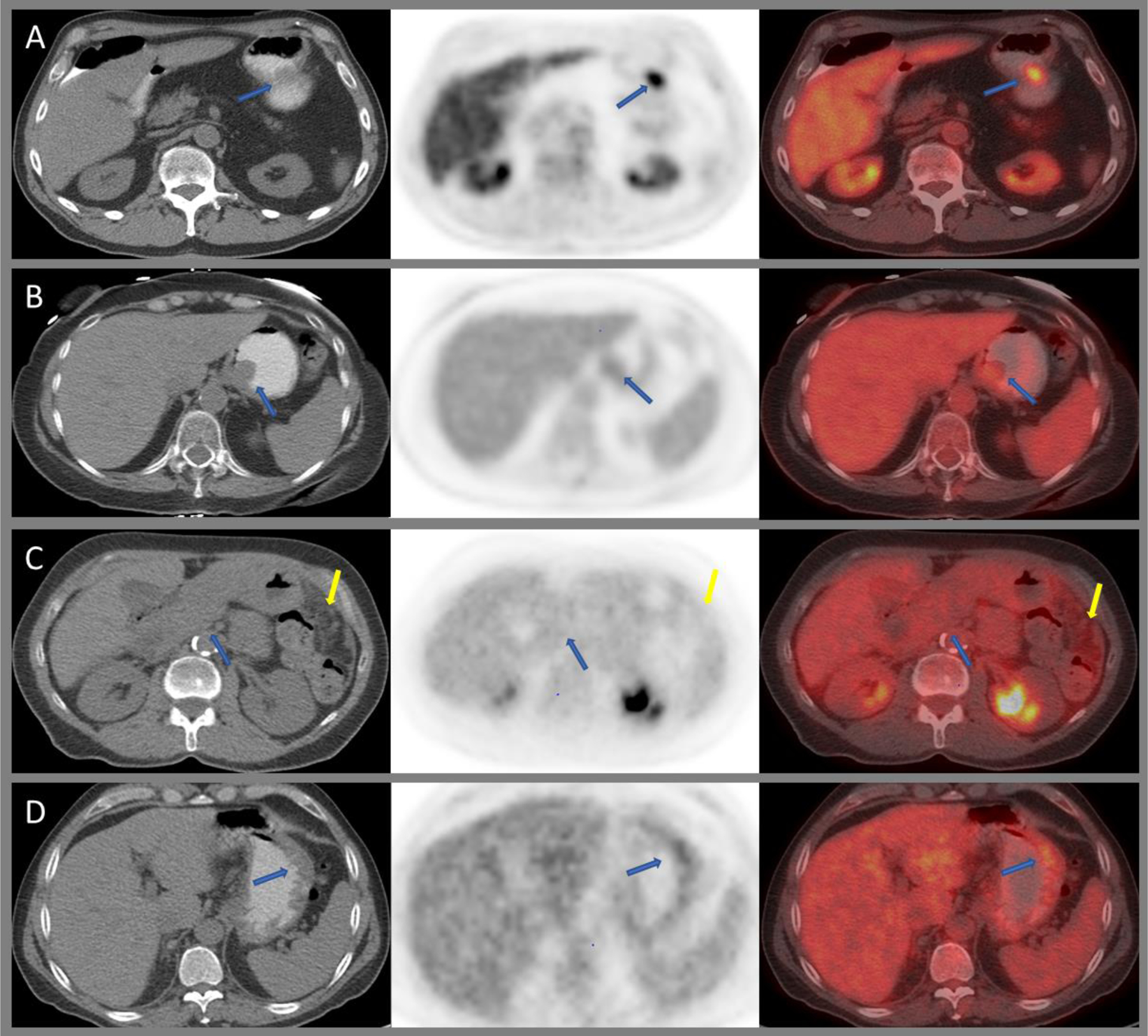
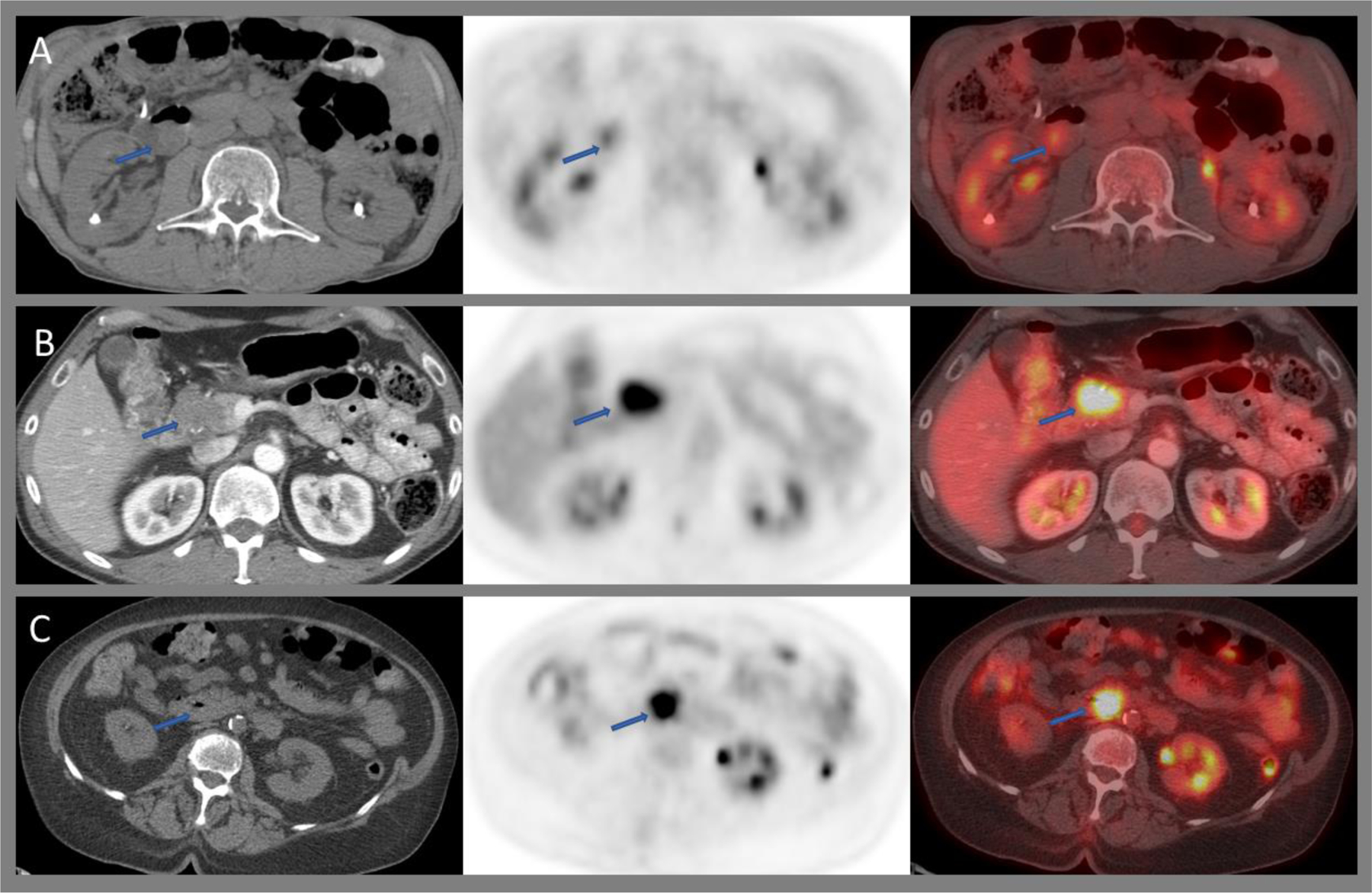
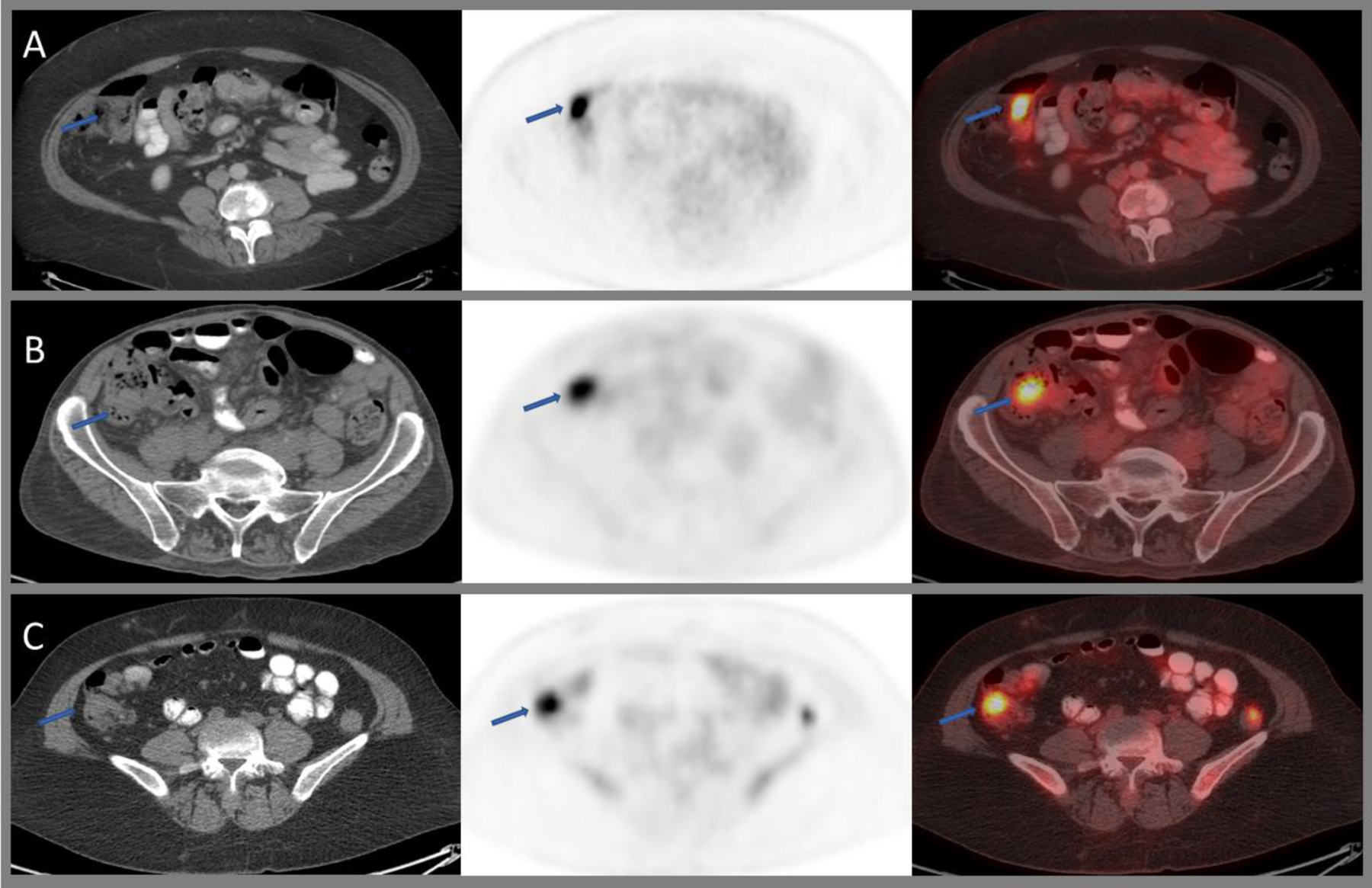
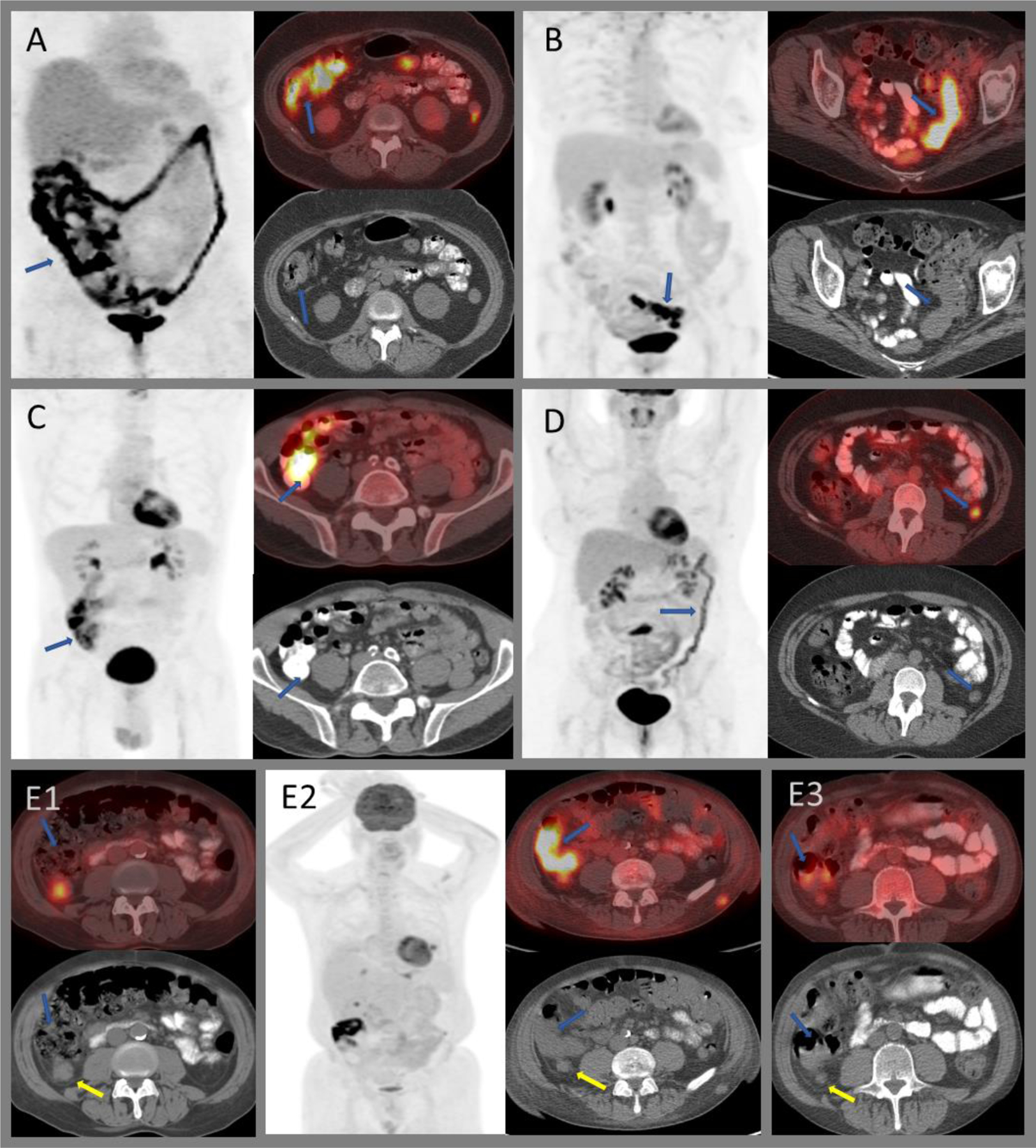
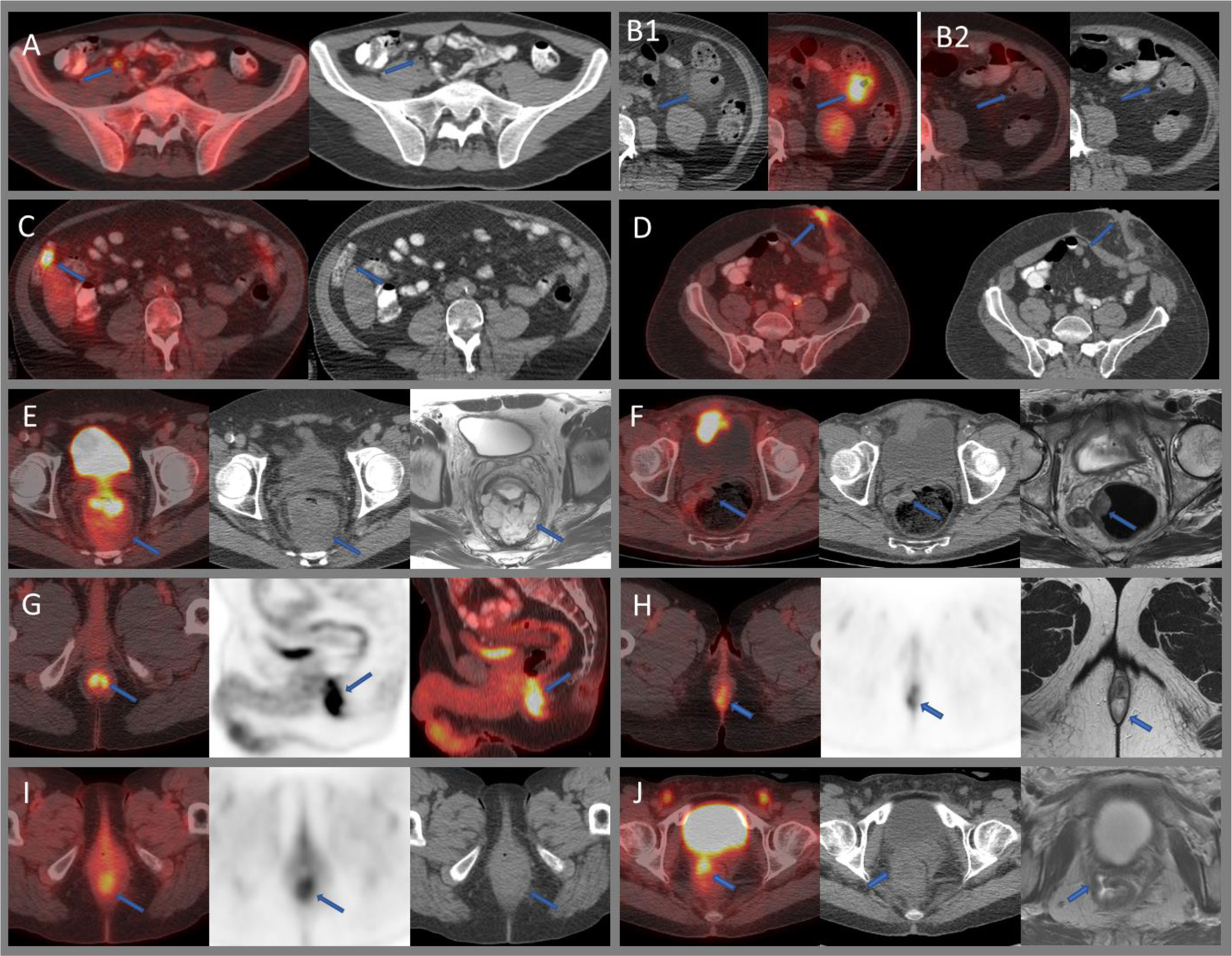
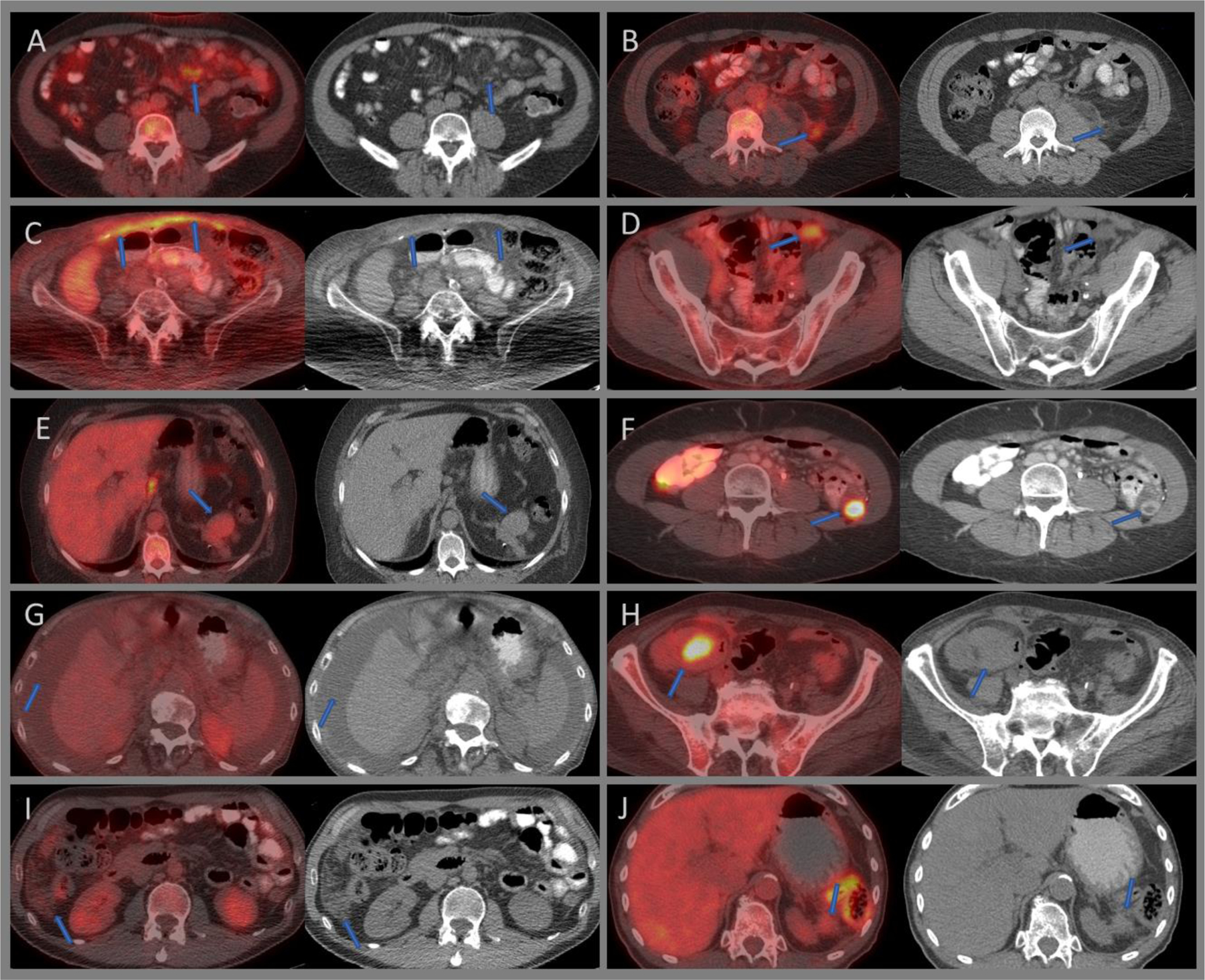
In the past two decades, PET/CT has become an essential modality in oncology increasingly used in the management of gastrointestinal (GI) cancers. Most PET/CT tracers used in clinical practice show some degree of GI uptake. This uptake is quite variable and knowledge of common patterns of biodistribution of various radiotracers is helpful in clinical practice. 18F-Fluoro-Deoxy-Glucose (FDG) is the most commonly used radiotracer and has quite a variable uptake within the bowel. 68Ga-Prostate specific membrane antigen (PSMA) shows intense uptake within the proximal small bowel loops. 11C-methyl-L-methionine (MET) shows high accumulation within the bowels, which makes it difficult to assess bowel or pelvic diseases. One must also be aware of technical artifacts causing difficulties in interpretations, such as high attenuation oral contrast material within the bowel lumen or misregistration artifact due to patient movements. It is imperative to know the common variants and benign diseases that can mimic malignant pathologies. Intense FDG uptake within the esophagus and stomach may be a normal variant or may be associated with benign conditions such as esophagitis, reflux disease, or gastritis. Metformin can cause diffuse intense uptake throughout the bowel loops. Intense physiologic uptake can also be seen within the anal canal. Segmental bowel uptake can be seen in inflammatory bowel disease, radiation, or medication induced enteritis/colitis or infection. Diagnosis of appendicitis or diverticular disease requires CT correlation, as normal appendix or diverticulum can show intense uptake. Certain malignant pathologies are known to have only low FDG uptake, such as early-stage esophageal adenocarcinoma, mucinous tumors, indolent lymphomas, and multicystic mesotheliomas. Response assessment, particularly in the neoadjuvant setting, can be limited by post-treatment inflammatory changes. Post-operative complications such as abscess or fistula formation can also show intense uptake and may obscure underlying malignant pathology. In the absence of clinical suspicion or rising tumor marker, the role of FDG PET/CT in routine surveillance of patients with GI malignancy is not clear.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures
References
-
- Howlader N, Noone AM, Krapcho M et al. SEER Cancer Statistics Review, 1975–2017, National Cancer Institute. Bethesda, MD. In, https://seercancergov/csr/1975_2017/, based on November 2019. SEER data submission, posted to the SEER web site, April 2020
-
- Beyer T, Townsend DW, Brun T et al. A combined PET/CT scanner for clinical oncology. J Nucl Med 2000; 41: 1369–1379 - PubMed
-
- Israeli RS, Powell CT, Corr JG et al. Expression of the prostate-specific membrane antigen. Cancer Res 1994; 54: 1807–1811 - PubMed
-
- Kinoshita Y, Kuratsukuri K, Landas S et al. Expression of prostate-specific membrane antigen in normal and malignant human tissues. World J Surg 2006; 30: 628–636 - PubMed
-
- Krohn T, Verburg FA, Pufe T et al. [(68)Ga]PSMA-HBED uptake mimicking lymph node metastasis in coeliac ganglia: an important pitfall in clinical practice. Eur J Nucl Med Mol Imaging 2015; 42: 210–214 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
