

Catheter-based interventions versus medical and surgical approaches in acute pulmonary embolism
- PMID: 33965609
- PMCID: PMC9048149
- DOI: 10.1016/j.jvsv.2021.02.015
Catheter-based interventions versus medical and surgical approaches in acute pulmonary embolism
Abstract
Objective: Catheter-based intervention (CBI) has become an increasingly popular option for treating pulmonary embolism (PE); however, the real benefits are unknown. The purpose of the present study was to compare the outcomes of patients treated with CBI with the outcomes of those treated with medical or surgical approaches.
Methods: We performed a retrospective analysis of patients admitted from October 2015 to December 2017 with a diagnosis of acute PE. We compared patients aged ≥18 years with a diagnosis of acute PE treated with CBI against a control group identified by propensity score matching. The control group was divided into those who had undergone surgical pulmonary embolectomy (SPE) as the surgical group and those who had not undergone SPE as the medical group. The primary outcome was mortality (in-hospital and overall mortality). The secondary outcomes were major bleeding, length of hospital stay, thrombus resolution, right ventricle improvement in systolic function and dilatation, and recurrent PE.
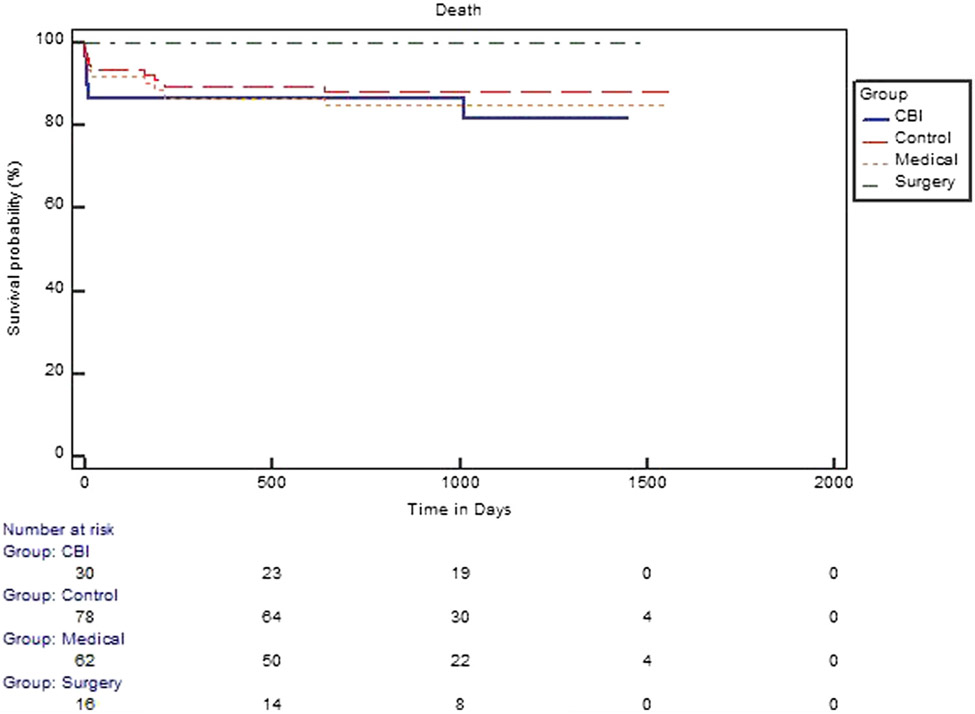
Results: Of the 108 patients, 30 were in the CBI group and 78 were in the control group (62 in the medical group and 16 in the surgical group). The patient characteristics on admission were similar, except for the body mass index, which was greater in the CBI group (P = .03). No difference was found in clinical severity, clot burden, right ventricle function, or biomarkers. Recurrent PE was less frequent in the CBI group than in the medical group (0% vs 6.4%). Otherwise, no significant differences were found in the outcomes between the CBI and medical groups. When CBI was compared with the surgical group, SPE was associated with improved mortality (0% vs 16.6%) but a longer median length of hospital stay (median, 7 days; interquartile range, 3-12 days; vs median, 8 days; interquartile range, 6.5-17 days).
Conclusions: The use of CBI reduced the number of recurrent PE events compared with the medically treated patients; however, the mortality was higher than that in the surgical group.
Keywords: Anticoagulation; Catheter-based therapies; Pulmonary embolism; Surgical pulmonary embolectomy.
Copyright © 2021 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Author conflict of interest: none.
Figures
References
-
- Beckman MG, Hooper WC, Critchley SE, Ortel TL. Venous thromboembolism: a public health concern. Am J Prev Med 2010;38(Suppl): S495–501. - PubMed
-
- Kucher N, Rossi E, De Rosa M, Goldhaber SZ. Massive pulmonary embolism. Circulation 2006;113:577–82. - PubMed
-
- Kearon C, Akl EA, Ornelas J, Blaivas A, Jiménez D, Bounameaux H, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest 2016;149:315–52. - PubMed
-
- Chatterjee S, Chakraborty A, Weinberg I, Kadakia M, Wilensky R, Sardar P, et al. Thrombolysis for pulmonary embolism and risk of all-cause mortality, major bleeding, and intracranial hemorrhage: a meta-analysis. JAMA 2014;311:2414–21. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
